Exabis Library
Welcome to the e-CCO Library!
With a growing prevalence of inflammatory bowel disease (IBD) in elderly patients, there is a clinical requirement to understand the impact of treatment in this population.1 Filgotinib (FIL) is an oral Janus kinase 1 preferential inhibitor. This post hoc analysis of data collected in the phase 2b/3 SELECTION programme evaluated the efficacy and safety of FIL in patients with ulcerative colitis (UC) stratified by age.
MethodsThe SELECTION programme includes two Induction Studies, a Maintenance Study (NCT02914522) and a long-term extension (LTE) study (NCT02914535). Adults aged 18–75 years with moderately to severely active UC were randomized 2:2:1 to receive FIL 200 mg or 100 mg or placebo once daily for 11 weeks. Responders at week 10 were re-randomized 2:1 to continue assigned FIL treatment or placebo from week 11–58. In LTE, patients with disease worsening and those completing week 58 continued assigned treatment before receiving open-label FIL. We assessed the efficacy and safety of FIL at any dose in the overall cohort of SELECTION and LTE, stratified into five age groups: <30, ≥30–<40, ≥40–<50, ≥50–<60 and ≥60 years. Clinical remission was evaluated at week 10 and pMCS remission was assessed at week 10, 58 and LTE weeks 2, 4, 12 and 24. Exposure-adjusted incidence rates (EAIRs) were calculated for adverse events (AEs). A data cut-off of 28 February 2020 was used.
ResultsBaseline disease activity and previous and concomitant treatments were comparable across age groups in each treatment arm. While there were fewer patients in the ≥60 years group, patient distribution was similar in all other age groups. FIL induced clinical (~16%) and pMCS (~36%) remission in similar proportions of patients across all age groups at week 10 (Figure 1). At week 58, pMCS remission was achieved in ~53% of FIL-treated patients across age groups (Figure 2). In LTE, the proportion of FIL-treated patients in pMCS remission generally increased with time and remained similar across all age groups (Figure 3). FIL-treated patients aged ≥60 years had higher EAIRs of any AE, infections, herpes zoster, malignancies, NMSC and MACE than younger patients (Table). One thromboembolic event occurred in a FIL-treated patient aged <30 years. Three deaths related to cardiovascular disease occurred in FIL-treated patients aged ≥50 years.



These findings suggest FIL is efficacious in inducing and maintaining symptomatic remission and could have an acceptable safety profile in adults with UC of all ages, including ≥60 years old. Age-related increases in incidences of certain AEs might be expected in patients with IBD; however, the number of patients ≥60 years limits comparison of these data with reported rates.
1Zammarchi et al. BMC Gastroenterol 2020;20;147
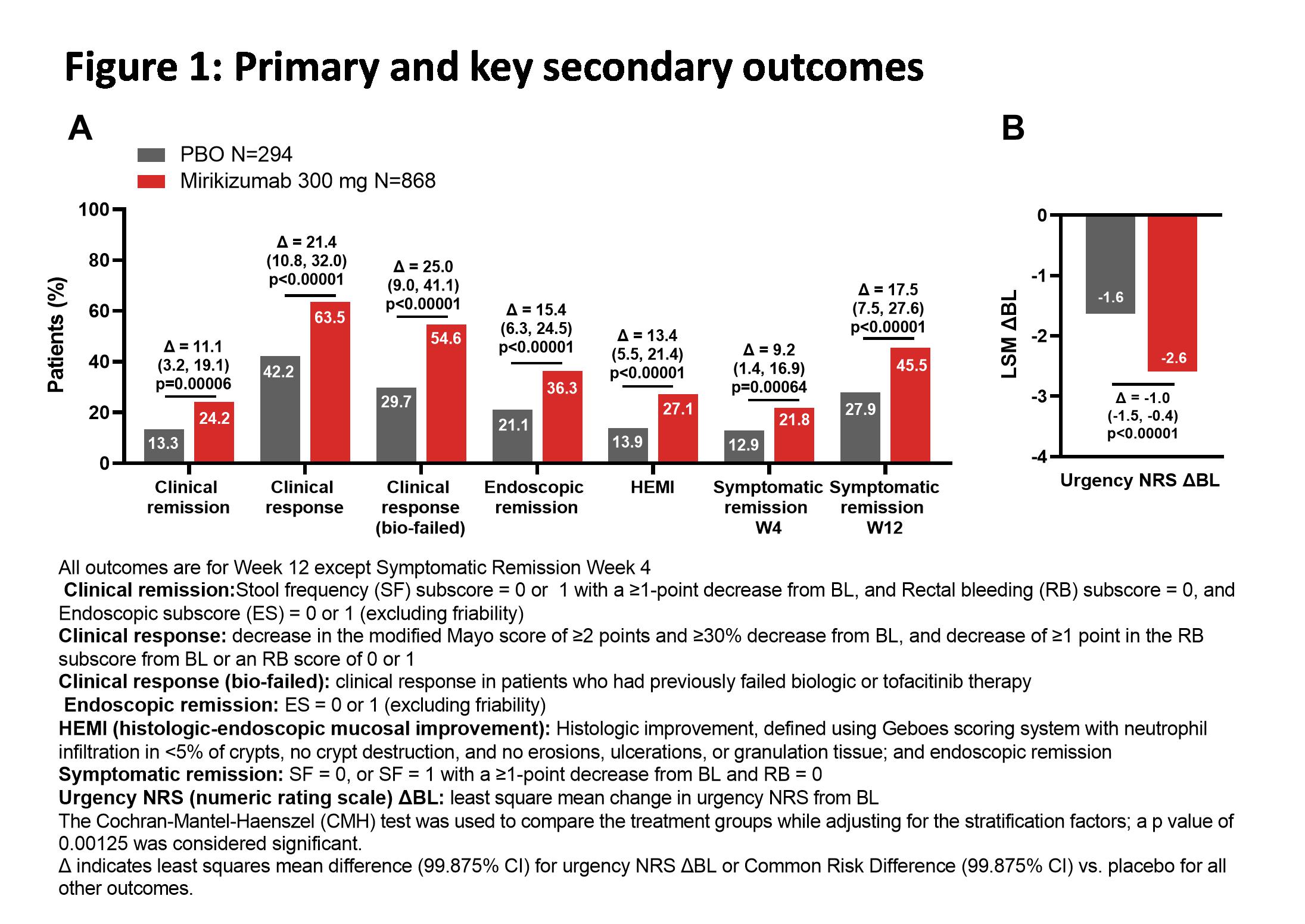
Anti-IL23p19 inhibitors are emerging as promising treatment options for ulcerative colitis (UC). Mirikizumab (miri) is a humanized, IgG4 monoclonal antibody directed against the p19 subunit of IL-23, a key mediator in the pathogenesis of inflammatory bowel diseases. We assessed the induction efficacy and safety of miri with a Phase 3, multi-center, randomized, parallel-arm, double-blind, placebo (PBO)-controlled trial (LUCENT 1; NCT03518086) in patients with moderately to severely active UC (Modified Mayo Score 4-9 points and centrally read Mayo endoscopic subscore ≥2) who had inadequate response, loss of response, or intolerance to corticosteroids, immunosuppressants, biologic therapies, or tofacitinib.
MethodsAdult patients (N=1281) were randomized in a 3:1 ratio to receive blinded intravenous administration of 300 mg miri or PBO every 4 weeks for 12 weeks. Randomization was stratified by biologic failure status, baseline (BL) corticosteroid use, BL disease activity as measured by modified Mayo score, and world region. The primary objective was to test the hypothesis that miri was superior to PBO in inducing clinical remission at Week 12. Key secondary objectives were clinical response, endoscopic remission, symptomatic remission, clinical response in biologic-failed patients, histologic-endoscopic mucosal improvement, and improvement in bowel urgency at Week 12 (see Figure for endpoint definitions). Mixed Model for Repeated Measures was used to assess urgency; the Cochran-Mantel-Haenszel test, with missing data imputed as nonresponse, was used to assess all other outcomes.
ResultsBL characteristics were balanced across the two treatment groups. A significantly greater proportion of patients treated with miri achieved clinical remission at Week 12 (Miri: 24.2%; PBO: 13.3%; Δ=11.1 [99.875%CI: 3.2, 19.1]; p=0.00006). Miri-treated patients achieved all key secondary endpoints, including a significantly greater average reduction in bowel urgency severity compared to PBO (p<0.00001). The frequencies of treatment-emergent adverse events in miri-treated patients were similar to PBO. There were numerically fewer serious adverse events (Miri: 27 [2.8%], PBO: 17 [5.3%]) and discontinuations due to adverse events (Miri: 15 [1.6%], PBO: 23 [7.2%]) in miri-treated patients compared to PBO. There were 2 colon malignancies in the miri arm (0.2%) and no deaths during the treatment period.
In this phase 3 UC study, 300mg miri IV demonstrated statistically significant and clinically meaningful improvements vs PBO in all primary and key secondary endpoints across clinical, endoscopic, histologic, and symptomatic measures, with an acceptable safety profile.

In Crohn’s disease (CD), disease location affects treatment outcomes.1 This post hoc analysis assessed the efficacy of risankizumab (RZB), an interleukin 23 p19 inhibitor, by disease location.
MethodsIn ADVANCE (NCT03105128) and MOTIVATE (NCT03104413), patients with moderately to severely active CD and intolerance or inadequate response to conventional and/or biologic therapy (ADVANCE) or to biologic therapy (MOTIVATE) received intravenous (IV) RZB induction therapy or placebo (PBO) for 12 weeks. Patients achieving clinical response to IV RZB induction were re-randomised in a maintenance study (FORTIFY, NCT03105102) to receive subcutaneous (SC) RZB or SC PBO (ie, withdrawal) for 52 weeks. This post hoc analysis included patients who received RZB 600 mg IV in either ADVANCE or MOTIVATE and patients who received RZB 360 mg SC in FORTIFY. Clinical and endoscopic outcomes were evaluated in patient subgroups stratified by CD location at baseline (ileal only, colonic only, ileal-colonic) using non-responder imputation incorporating multiple imputation to handle missing data due to COVID-19.
ResultsAt week 12, significantly greater proportions of patients receiving RZB 600 mg IV achieved the co-primary endpoints CD Activity Index (CDAI) clinical remission and endoscopic response vs PBO in the colonic only (n = 190) and ileal-colonic (n = 252) subgroups (P < .001; Figure 1A–1B). At week 12, statistically higher proportions of RZB-treated patients achieved the composite endpoint CDAI clinical remission and endoscopic response, as well as endoscopic remission in the colonic only and ileal-colonic subgroups vs PBO (P < .001; Figure 1C–1D). At week 52, significantly greater proportions of patients receiving RZB 360 mg SC achieved the co-primary endpoints CDAI clinical remission and endoscopic response, composite CDAI clinical remission and endoscopic response, and endoscopic remission vs withdrawal (PBO SC) in the colonic only (n = 59) and ileal-colonic (n = 67) subgroups (P ≤ .05; Figure 2A–2D). In patients with endoscopic remission after 12 weeks of IV RZB (week 0 of maintenance), significantly more RZB-treated patients achieved sustained endoscopic remission at week 52 vs withdrawal (PBO SC) in the colonic only and ileal-colonic subgroups (P ≤ .01; Figure 2E). At weeks 12 and 52, efficacy rates were numerically lower in ileal only CD relative to colonic only and ileal-colonic CD. Results for ileal only CD are limited by the small number of patients in the subgroup (induction, n = 85; maintenance, n = 15).

RZB induction and maintenance therapy was effective in patients with moderately to severely active CD with greater benefits observed in patients with any colonic involvement.
The efficacy and safety of 12 weeks of induction and 52 weeks of maintenance treatment with risankizumab (RZB), an interleukin 23 p19 inhibitor, in patients with moderately to severely active Crohn’s disease (CD) was previously demonstrated in 3 phase 3 trials (ADVANCE, MOTIVATE, and FORTIFY). We investigated outcomes in patients with inadequate response to subcutaneous (SC) RZB or SC placebo (PBO) treatment and required RZB rescue therapy during maintenance.
MethodsIn FORTIFY, a phase 3, double-blind, re-randomised responder withdrawal, maintenance study (NCT03105102), patients that responded to 12 weeks of RZB IV induction received RZB 180 mg SC, RZB 360 mg SC, or PBO (ie, withdrawal) every 8 weeks for 52 weeks. Starting at week 16, patients with inadequate response, defined as average daily stool frequency [SF] ≥ 3.3 and/or average daily abdominal pain score [APS] ≥ 1.5 as well as high‑sensitivity C-reactive protein ≥ 5 mg/L and/or faecal calprotectin ≥ 250 μg/g; or Simple Endoscopic Score for CD (SES-CD) ≥ 6 (≥ 4 for isolated ileal disease), excluding the narrowing component as scored by the site Investigator, were eligible to receive open-label rescue therapy (1 dose of intravenous [IV] RZB 1200 mg, followed by RZB 360 mg SC every 8 weeks). Up to 2 rescue therapy visits ≥ 16 weeks apart were permitted. Efficacy at week 52 was assessed in the intent-to-treat population using nonresponder imputation for missing data. Patients were also considered nonresponders when maximum equivalent steroid dose exceeded the dose used at baseline or if patients initiated any new steroids. Safety was assessed throughout the study.
ResultsIn the maintenance study, a greater proportion of patients in the withdrawal (PBO SC) arm (40.2% [66/164]) were administered RZB rescue therapy vs RZB 180 mg SC (24.2% [38/157]) and RZB 360 mg SC (21.3% [30/141]; Figure A); most patients (71.1%–81.8%) required 1 rescue visit, and 16.7%–26.3% required 2 visits.Median time to first RZB rescue therapy was 178 days for the withdrawal (PBO SC) group, 179 days for the RZB 180 mg SC group, and 154 days for the RZB 360 mg SC group. At week 52, 52.5%–75.0% of patients who received RZB rescue therapy achieved SF/APS clinical response (Figure B), and 20.0–36.4% of patients who received rescue therapy achieved clinical remission (per CDAI or SF/APS) and/or endoscopic response (Figures C-E).The safety profile of RZB in CD has previously been reported.
RZB rescue therapy (one dose of RZB 1200 mg IV followed by RZB 360 mg SC every 8 weeks) may be beneficial to patients with moderately to severely active CD experiencing inadequate response to or interruption in RZB maintenance treatment.
STARDUST is a phase 3b randomized trial comparing two therapeutic strategies with ustekinumab (UST) in patients (pts) with Crohn’s disease (CD): treat-to-target (T2T) using early endoscopic assessment vs standard of care (SoC). Results from the Week (W)48 and long-term extension (LTE) (W48 to W104) were published previously.1,2 Here we explore the efficacy of the T2T approach in modifying disease course with UST by analyzing time-to-disease modifying (DM) event up to W104.
MethodsAdult pts with moderate–severe active CD, received iv, weight-based UST ~6mg/kg at W0; then sc UST 90mg at W8. At W16, pts with ≥70-point reduction in CD Activity Index were randomized 1:1 to either T2T or SoC and received sc UST 90mg, every 12W/8W (up to 4W in the T2T arm), as per the protocol. From W48, eligible pts could continue to receive sc UST up to W104 with further protocol-guided dose adjustment. DM events were recorded through W48 and W104 starting at randomization, and time-to-event analysis was performed for pts in both arms. DM events are represented by combined bowel damage events (defined as the development of new strictures/fistulae or the occurrence of an intra-abdominal abscess) or CD-related hospitalizations or surgeries based on the adverse event analysis. Time-to-first bowel damage event, CD-related surgery, hospitalization, hospitalization or surgery was analyzed separately; Kaplan–Meier (K–M) curves with corresponding hazard ratios (HRs) and 95% confidence intervals (CIs) are shown here.
ResultsOf 440 pts randomized to either T2T or SoC at W16, 74 discontinued before W48. Of the remaining 366 pts completing W48, 43 discontinued and did not enter LTE. At W48, 323 pts entered LTE; 20.1% of these pts discontinued before completing W104. HRs (95% CI) for time-to-first DM event from randomization through W48 and W104 are shown in Table 1, suggesting a numeric benefit in favour of the T2T arm. The separation of the K–M curves for time-to-first DM eventbetween the two arms was apparent at W48 and continued up to W104, without significant difference (Figure 1a and b). 


In STARDUST, with UST, starting at W48, numerically less DM events were observed in the T2T arm, mainly driven by the lower number of CD-related hospitalizations and bowel damage events, potentially linked to numerically higher proportion of endoscopic responders at W48.1 These results advocate for an optimized T2T approach using strictly defined targets like endoscopic response, on top of clinical and biomarkers, to facilitate decision making in clinical practice.
1Danese S, et al. United European Gastroenterol J. 2020;8:1264–1265 (Abstract LB11).
2Peyrin-Biroulet L, et al. United European Gastroenterol J. 2021;9 (Suppl 1).