Exabis Library
Welcome to the e-CCO Library!
The oral, selective Janus kinase inhibitor upadacitinib (UPA) has demonstrated efficacy as induction and maintenance therapy in patients with moderately to severely active Ulcerative Colitis (UC) in a Phase 3 clinical programme comprising two identical induction trials (U-ACHIEVE Induction [NCT02819635] and U-ACCOMPLISH [NCT03653026]) and a maintenance study (U-ACHIEVE Maintenance). This analysis assessed the impact of baseline corticosteroid (CS) use on the efficacy and safety of UPA in patients in these trials.
MethodsPatients were randomised 2:1 to UPA 45 mg once daily (QD) or placebo (PBO) for 8 weeks. Patients who achieved a clinical response at Week 8 were re-randomised 1:1:1 to UPA 15 mg QD, UPA 30 mg QD or PBO for 52 weeks. Here, we report induction and maintenance endpoints and safety data stratified by baseline CS use.
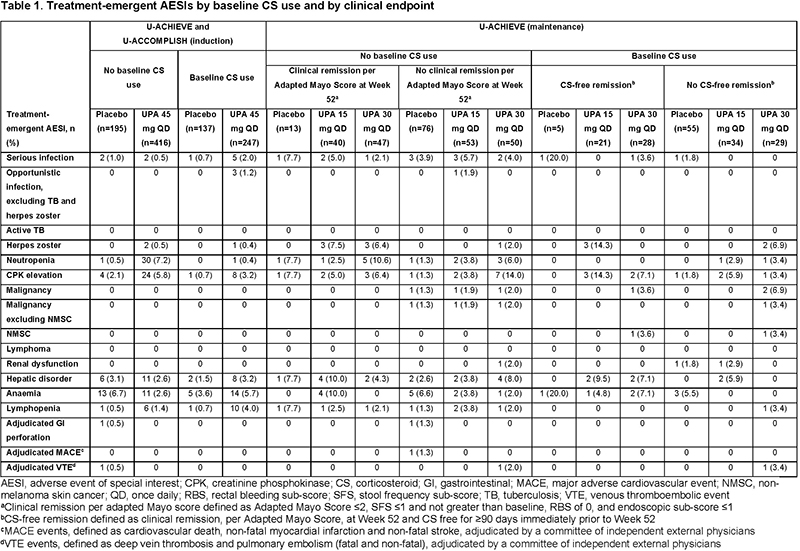
ResultsBaseline demographics and disease characteristics were generally well balanced across treatment groups, regardless of baseline CS use. Clinical remission rates among patients receiving UPA 45 mg induction therapy did not differ by baseline CS use (Figure 1A). In the induction period, rates of treatment-emergent adverse events of special interest (AESI), including serious and opportunistic infections, were increased in the UPA 45 mg plus baseline CS group compared with the PBO and UPA without baseline CS groups (Table 1). In the maintenance study, CS tapering was mandated. CS-free remission at Week 52 (defined as clinical remission, per Adapted Mayo Score, and CS free for ≥90 days immediately prior to Week 52) was significantly increased with UPA 30 and 15 mg compared with PBO (both p<0.001; Figure 1B). Among patients receiving UPA maintenance, rates of treatment-emergent AESIs in the baseline CS versus no baseline CS groups were 33% versus 39% and 27% versus 35% in the UPA 30 mg and UPA 15 mg groups, respectively. Malignancy, major adverse cardiovascular events, venous thromboembolic events, and serious and opportunistic infections were reported infrequently in patients receiving UPA (Table 1).
This post hoc analysis suggests that, in patients with moderately to severely active UC, UPA is superior to PBO in conferring CS-free remission. Baseline CS use was not associated with any apparent efficacy benefit and carried a potential increased safety risk. These results suggest that achieving early disease control with UPA and without CS use is an optimal treatment strategy for this population.
Patients with IBD show distinct antibody responses, particularly against microbiota. However, a comprehensive overview of the antibody epitope repertoire in IBD is lacking. Here, we characterized serum antibody responses in patients with IBD and population controls using a high-throughput phage-displayed immunoprecipitation sequencing (PhIP-seq) workflow and associated these to disease phenotypes and the faecal microbiome.
MethodsPhIP-seq was leveraged to characterise antibody responses against 344,000 rationally selected peptide antigens in 497 patients with IBD which were compared with 1,326 individuals from a population-based cohort (Fig. 1A-B). Antibody profiles were linked to 23 IBD-specific clinical features such as disease location and surgical history and to faecal microbiota composition (Fig. 1C).
Patients with IBD demonstrated distinct antibody epitope repertoires compared with individuals from the general population, with 373 differentially abundant antibody-bound peptides (202 overrepresented, 171 underrepresented) belonging to bacterial flagellins (69), virulence factors (102), other antigens of both commensal and pathogenic bacteria (90) as well as viruses (67) and food proteins (24) (Figure 2). In particular, antibody responses against bacterial flagellins, many of which belong to Lachnospiraceae bacteria (e.g. Roseburia spp.), but also Eubacterium spp. and pathogens (e.g. Legionella, Clostridium, Burkholderia) dominated in patients with Crohn's disease (CD), and were associated with ileal disease involvement and more complicated disease behaviour (e.g. fibrostenotic disease, surgical history) as well as anti-Saccharomyces cerevisiae antibody positivity. Furthermore, many other antigens were newly identified, e.g. decreased responses to E. coli virulence factors and genome polyproteins of enteroviruses, and increased responses to food antigens (wheat, barley) and autoantigens (particularly collagen type I and VI). Antibody epitope repertoires were able to accurately discriminate CD from population controls (area under the curve [AUC]=0.88, test set evaluation), showing very high discriminative performance (positive and negative predictive value of 72% and 93%, respectively, representing predicted classes in test set) (Fig. 3A-C), which was less accurate for ulcerative colitis (UC) (Fig. 3D-F).

 Conclusion
ConclusionThis study demonstrates the size, diversity and complexity of systemic antibody epitope repertoires in patients with IBD compared to controls, showing that distinct clinical phenotypes of IBD are characterized by unique antibody signatures. PhIP-seq is a powerful tool for identifying systemic immune-based biomarkers and exposing novel immunological targets in immune-mediated inflammatory diseases like IBD.
Patients with IBD show distinct antibody responses, particularly against microbiota. However, a comprehensive overview of the antibody epitope repertoire in IBD is lacking. Here, we characterized serum antibody responses in patients with IBD and population controls using a high-throughput phage-displayed immunoprecipitation sequencing (PhIP-seq) workflow and associated these to disease phenotypes and the faecal microbiome.
MethodsPhIP-seq was leveraged to characterise antibody responses against 344,000 rationally selected peptide antigens in 497 patients with IBD which were compared with 1,326 individuals from a population-based cohort (Fig. 1A-B). Antibody profiles were linked to 23 IBD-specific clinical features such as disease location and surgical history and to faecal microbiota composition (Fig. 1C).
Patients with IBD demonstrated distinct antibody epitope repertoires compared with individuals from the general population, with 373 differentially abundant antibody-bound peptides (202 overrepresented, 171 underrepresented) belonging to bacterial flagellins (69), virulence factors (102), other antigens of both commensal and pathogenic bacteria (90) as well as viruses (67) and food proteins (24) (Figure 2). In particular, antibody responses against bacterial flagellins, many of which belong to Lachnospiraceae bacteria (e.g. Roseburia spp.), but also Eubacterium spp. and pathogens (e.g. Legionella, Clostridium, Burkholderia) dominated in patients with Crohn's disease (CD), and were associated with ileal disease involvement and more complicated disease behaviour (e.g. fibrostenotic disease, surgical history) as well as anti-Saccharomyces cerevisiae antibody positivity. Furthermore, many other antigens were newly identified, e.g. decreased responses to E. coli virulence factors and genome polyproteins of enteroviruses, and increased responses to food antigens (wheat, barley) and autoantigens (particularly collagen type I and VI). Antibody epitope repertoires were able to accurately discriminate CD from population controls (area under the curve [AUC]=0.88, test set evaluation), showing very high discriminative performance (positive and negative predictive value of 72% and 93%, respectively, representing predicted classes in test set) (Fig. 3A-C), which was less accurate for ulcerative colitis (UC) (Fig. 3D-F).
ConclusionThis study demonstrates the size, diversity and complexity of systemic antibody epitope repertoires in patients with IBD compared to controls, showing that distinct clinical phenotypes of IBD are characterized by unique antibody signatures. PhIP-seq is a powerful tool for identifying systemic immune-based biomarkers and exposing novel immunological targets in immune-mediated inflammatory diseases like IBD.
The burden of inflammatory bowel disease (IBD) in health care is high and the incidence and prevalence rates of IBD in Finland are among the highest in the world. Our aim was to assess the actual incidence and the trends of IBD in Finland during 2000-2020 using nationwide registry-based data. We also estimated the nationwide prevalence of IBD in 2000 and 2020.
MethodsThis study included patients to whom IBD reimbursement was newly attributed between January 1, 2000 and December 31, 2021. Data were retrieved from the Social Insurance Institution of Finland. Incidence and prevalence rates were calculated by dividing the number of annual new IBD cases by the size of the population at risk during each calendar year.
ResultsA total of 42,498 new IBD cases were identified during years 2000-2020; 31,372 with ulcerative colitis (UC) and 11,126 with Crohn’s disease (CD).The crude annual incidence per 100,000 increases in CD from 7.5 to 13.4 (IRR 1.02, CI 1.019 - 1.025) and in UC from 20.4 to 34.7 (IRR 1.03, CI 1.023 - 1.027) (Fig. 1). The crude prevalence of IBD increases from 376 to 972 per 100,000 (PRR 1.05, CI 1.046-1.047).Men have significantly higher incidence than women in UC (IRR 1.26, CI 1.228-1.284). In contrast, there is no difference between genders among CD patients (IRR 0.98, CI 0.95-1.02). In UC, the peak incidence occurs in the age group 25-29 (Fig. 2), whereas in CD, the incidence is
highest in slightly younger patients (Fig. 3).
Figure 1. Incidence of ulcerative colitis and Crohn`s disease in Finland during 2000-2020
Figure 2. Annual incidence of UC by age groups during 2000-2020
Figure 3. Annual incidence of CD by age groups during 2000-2020
During the first two decades of the 21st century, the incidence of UC and CD continues to increase in Finland, and almost one percent of the population has IBD.
Current knowledge regarding the epidemiology of pouchitis is based on highly selected, mostly single-center, patient cohorts. Our objective was to prospectively determine the population-based incidence of pouchitis in patients with ulcerative colitis (UC) in the first 2 years after ileal pouch-anal anastomosis (IPAA) and analyze time trends of the incidence of pouchitis.
MethodsWe used national registries to establish a population-based cohort of all Danish patients undergoing proctocolectomy with IPAA UC between 1996 and 2018. The primary outcome was the development of pouchitis within the first 2 years after IPAA, evaluated by time period of IPAA. The period of IPAA was categorized as follows: 1996-2000 (pre-biologic-1), 2001-2005 (pre-biologic-2), 2006-2010 (early-anti-TNF), 2011-2014 (expanding anti-TNF), 2015-2018 (current biologic). Pouchitis was defined using a previously developed case-finding definition for use in administrative claims data. Kaplan Meier and Cox Proportional Hazard modeling were utilized in the evaluation of time to development of pouchitis.
ResultsWe identified 1,664 patients that underwent an IPAA for UC. The cumulative incidence of pouchitis in the 2 years after IPAA increased throughout the study period, from 40% in 1996-2000, (95% CI:35%-46%) to 55% in 2015-2018, (95% CI:48%-63%, Table 1). Patients undergoing surgery between 2015-2018 also demonstrated an increased risk of pouchitis compared to the earliest study period (1996-2000) after adjusting for sex, age, and socioeconomic status (Hazard Ratio [HR] 1.57, 95% CI:1.20-2.05, Table 2, Figure 1). In a separate model adjusting for the same clinical and demographic factors, there was no significant relationship between the preoperative use of anti-tumor necrosis factor alpha therapy use and the risk of pouchitis when evaluated in the entire population (HR 1.14, 95% CI:0.93-1.40) and when evaluated by time period of surgery.



This first population-based study demonstrated a 15% absolute and 38% relative increase in the incidence of pouchitis among patients undergoing surgery between 1996 and 2018, with the greatest cumulative incidence of pouchitis demonstrated in the most recent era (2015-2018). The striking increase in the incidence of pouchitis highlights the need for further research into causes and prevention of pouchitis.
Limited data is available of the outcome of inflammatory bowel disease (IBD) in patients with solid organ transplantation (SOT). The aim of our study was to describe the natural history of pre-existing IBD and de novo IBD after SOT.
A retrospective, observational, multi-centre, nationwide study was designed. IBD patients with SOT were included. We identified two separate cohorts: (1) patients with pre-existing IBD at the time of SOT and (2) patients without IBD at the time of SOT (de novo IBD). The primary outcome was IBD progression, defined by the escalation of medical treatment, surgical therapy for medically refractory IBD or IBD-related hospitalization during follow-up. Risk factors were identified using multivariate Cox proportional hazard analysis.
ResultsA total of 177 patients (106 pre-existing IBD and 71 de novo IBD) from 31 centres were included. Baseline characteristics are shown in Table 1. Eighty-six patients with IBD and SOT underwent liver transplantation, while 82 required renal, 4 lung, 3 heart, 1 liver/kidney and 1 pancreas/kidney transplantation.
Pre-existing IBD patients were followed-up over a median of 4.8 years (range 2.6-9.4). At the time of SOT, 61 patients (59.8%) were not under maintenance treatment or were treated with 5-aminosalicylates, 10 (9.8%) were on immunosuppressive therapy and 31 (30.4%) were receiving biological agents, of which 8 were on combo therapy. At the moment of SOT, only 8 patients (7.5%) had moderate IBD activity whereas the remaining patients were in remission. During follow-up 33.7% of patients with pre-existing IBD had disease progression, with a median time between SOT and IBD progression of 2.2 years (range 1.3-4.6). No differences between Crohn´s disease and ulcerative colitis were found (Figure 1).
The median time of follow-up in de novo IBD group was 5.1 years (range 2.1-8.2). In this cohort, 55.9% of patients had disease progression during follow-up (Figure 2), with a median time to flare of 1.9 years (range 0.8-3.9) from diagnosis.
In pre-existing IBD cohort, multivariate Cox-regression analysis identified active IBD at the time of SOT (HR=1.80; 95%CI: 1.14-2.84; p=0.012) and the presence of extraintestinal manifestations (HR=3.10; 95%CI: 1.47-6.54; p=0.003) as predictive factors of IBD progression after SOT.


One third of patients with pre-existing IBD have disease progression, needing medical therapy escalation, surgery or hospitalization after SOT. Active IBD at the time of SOT and the presence of extraintestinal manifestations were identified as risk factors for disease progression. In de novo IBD cohort, about half of patients showed disease progression during follow-up.
Monitoring of monoclonal antibody clearance has been hypothesised to be an appealing approach for predicting treatment outcomes in patients with inflammatory bowel diseases. We aimed to investigate the benefits of monitoring infliximab and ustekinumab clearance in patients with Crohn’s disease (CD) based on data from clinical trials.
MethodsData were obtained from patients with moderate-to-severe CD starting infliximab (n=108)1 or ustekinumab (n=80)2 therapy. Endoscopic remission (CD Endoscopic Index of Severity <3) and endoscopic response (≥50% decrease from baseline in simple endoscopic score for CD) were assessed at week (w)12 and w24 of infliximab and ustekinumab therapy, respectively. A priori prediction (based on covariate data only; at w0) and a posteriori prediction (Bayesian forecasting using measured drug concentrations; during treatment) were performed using previously built population pharmacokinetic models (NONMEM 7.5).3,4 Covariates of fecal calprotectin, albumin, CD activity index, and antibodies towards infliximab (ATIs) were used to estimate infliximab clearance. Albumin and body weight were used to estimate ustekinumab clearance.
ResultsPatients achieving endoscopic remission at w12 had significantly lower infliximab clearance and higher infliximab serum concentration at w2 and w6 of treatment (P <0.05, Table 1). Patients achieving endoscopic response at w24 had significantly lower ustekinumab clearance at w4 and w8, as well as a significantly larger reduction in clearance relative to w0 (P <0.05, Table 1). However, ustekinumab serum concentrations at w4 and w8 were similar between patients with and without endoscopic response (P >0.2, Table 1).
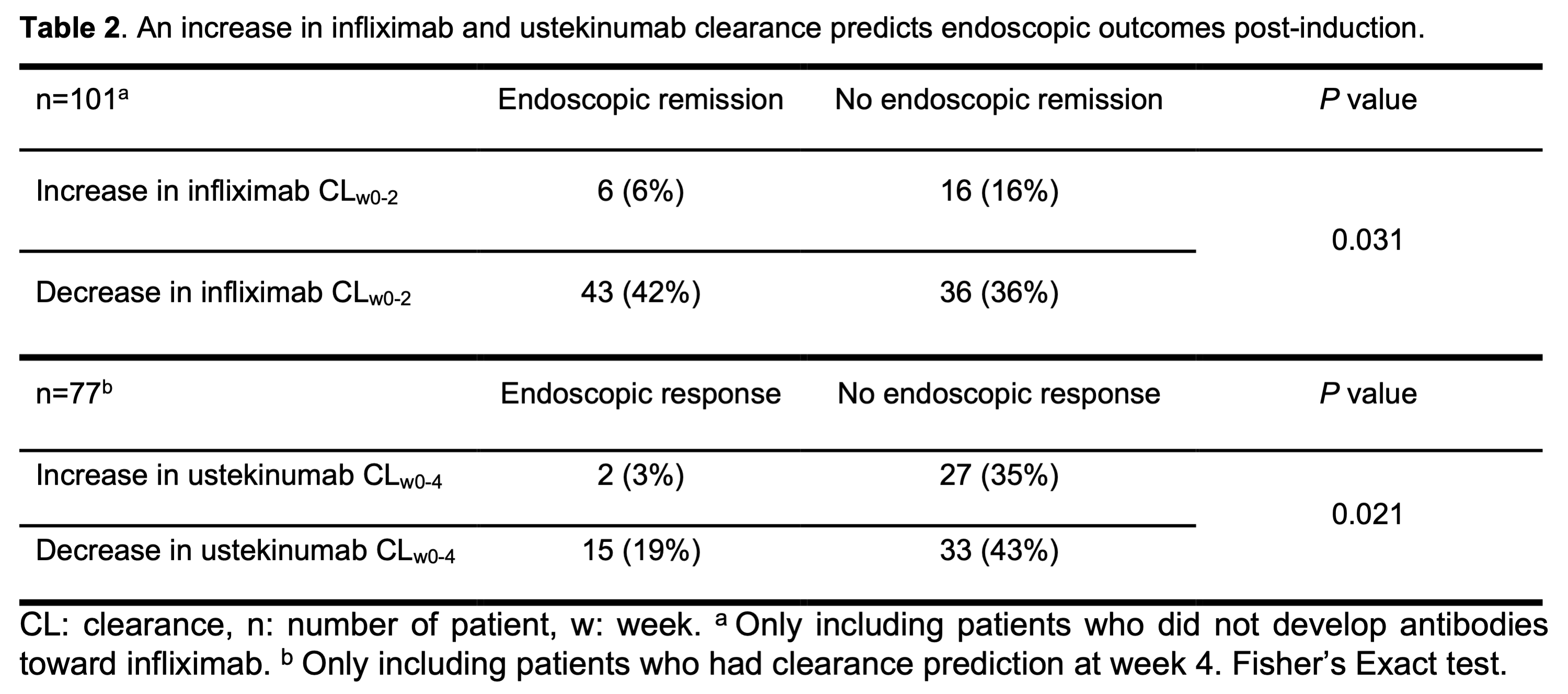
Most patients with an early increase in infliximab clearance (16/22; 73%) and ustekinumab clearance (27/29; 93%) did not reach the endoscopic endpoint (P <0.05; Table 2). However, a decrease in clearance was no guarantee for endoscopic remission during infliximab therapy (false predictive rate 46%) and response during ustekinumab therapy (false predictive rate 69%).
The infliximab clearance after start of induction therapy (at w2 and w6) was significantly higher in patients who developed ATIs during induction therapy (Figure 1).
Lower infliximab and ustekinumab clearance (absolute as well as relative to w0) early during induction predict more favourable endoscopic outcomes. In patients treated with ustekinumab, clearance monitoring may better predict endoscopic response at w24 as compared to standard therapeutic drug monitoring.
References
1. D'Haens et al.Gastroenterology 2018
2. Verstockt et al. J Crohns Colitis 2019.
3. Dreesen et al. Br J Clin Pharmacol 2021.
4. Wang et al. Br J Clin Pharmacol 2021.