Exabis Library
Welcome to the e-CCO Library!
Sphingosine-1-phosphate (S1P) receptor modulators may be associated with bradycardia and atrioventricular conduction delays. A previous analysis demonstrated first-dose ozanimod had minimal effects on cardiac function, including in patients (pts) with a known history of cardiovascular disease. This analysis evaluated long-term cardiac safety following continuous ozanimod treatment from the phase 3 ulcerative colitis (UC) True North trial and multiple sclerosis (MS) 12-mo SUNBEAM and 24-mo RADIANCE trials.
MethodsOzanimod 0.92 mg (equivalent to ozanimod HCl 1 mg)–treated pts from True North and pooled SUNBEAM/RADIANCE trials were included. In True North, pts in Cohort 1 received double-blind ozanimod or placebo and pts in Cohort 2 received open-label ozanimod in the induction period; in the maintenance period, pts with clinical response to ozanimod at 10 weeks were rerandomized to double-blind ozanimod or placebo. In True North, ECGs were monitored at screening, day 1, wk-10, and wk-52; heart rate (HR) was monitored at every visit. In the MS trials, ECGs were monitored at screening, baseline, day 15, and end of treatment (EOT); HR was monitored similarly at the beginning, then every 3 mo until EOT. Cardiac-related treatment-emergent AEs (TEAEs) were reported.
ResultsIn the UC trial, continuous ozanimod treatment was not associated with any clinically significant changes in HR or ECG. The incidence of cardiac-related TEAEs with ozanimod during induction in Cohorts 1 and 2 was low (Table). In maintenance, cardiac-related TEAEs were reported in 1.3% (3/230) of pts in the continuous ozanimod group (Table); incidence was numerically higher in ozanimod pts with (2 of 57 pts [3.5%]) versus without (1 of 173 pts [0.6%]) prior history of cardiovascular disease. Cardiac-related serious AEs (SAEs) were uncommon (angina pectoris, coronary artery stenosis, pericarditis in 1 patient each). In the pooled MS studies, no clinically significant HR or ECG changes were associated with chronic treatment up to mo 24. The incidence of cardiac-related TEAEs was low with ozanimod (Table); incidence was similar among pts with (6 of 171 pts [3.5%]) versus without (24 of 711 pts [3.4%]) prior history of cardiovascular disease. Two of 882 patients experienced cardiac-related SAEs resulting in hospitalization with ozanimod in the MS studies (asymptomatic sinus bradycardia [HR 44 bpm] and symptomatic supraventricular tachycardia).
ConclusionOzanimod had a manageable long-term cardiac safety profile with a low incidence of bradycardia and few serious long-term cardiac safety findings in the phase 3 UC and MS ozanimod trials.

The vast majority of patients with ulcerative colitis (UC) and Crohn’s disease (CD) who acquire coronavirus disease 2019 (COVID-19) survive the infection. Still, the long-term health consequences of COVID-19 are not well described in patients with underlying inflammatory bowel disease (IBD).
MethodsWe conducted a population-based study investigating the outcomes of COVID-19 among patients with UC and CD in Denmark. The Danish COVID-19 IBD Database is an extensive population-based database which prospectively monitors the disease course of laboratory-confirmed COVID-19 among patients with UC and CD. Severe COVID-19 was defined as COVID-19 necessitating intensive care unit admission, ventilator use, or death, while adverse COVID-19 was defined as requirement of COVID-19 related hospitalization. Sequelae following COVID-19 were defined as symptoms that developed during or after an infection consistent with COVID-19, were present for more than 12 weeks, and were not attributable to alternative diagnoses.
ResultsThe study included 319 patients with UC and 197 patients with CD from January 28th, 2020, to April 1st, 2021. Of these, a total of 137 (42.9%) and 85 (43.1%), respectively, participated in a subsequent investigation of post-COVID-19 sequelae after a median of 5.1 months (IQR 4.5-7.9) after infection (Table 1). An equal proportion of patients with UC (58 (42.3%)) and CD (39 (45.9%), p=0.60) reported persisting symptoms of COVID-19 for at least 12 weeks, consistent with the development of post-COVID-19 syndrome. The most common persisting patient-reported symptoms included fatigue (UC: 49 (35.8%), CD: 31 (36.5%), p=0.92), anosmia (UC: 37 (27.0%), CD: 25 (29.4%), p=0.70), ageusia (UC: 26 (19.0%), CD: 24 (28.2%), p=0.11), headache (UC: 19 (13.9%), CD: 16 (18.8%), p=0.32), dyspnea (UC: 19 (13.9%), CD: 16 (18.8%), p=0.32), and arthralgia (UC: 17 (12.4%), CD: 14 (16.5%), p=0.40) (Figure 1). Only discontinuation of immunosuppressive therapies for UC during COVID-19 (OR=1.50 (95% CI 1.07-10.22), p=0.01) and the severity of COVID-19 among patients with CD were independently associated with the long-term effects of COVID-19 (OR=2.76 (95% CI 1.05-3.90), p=0.04) (Tables 2-3).



 Conclusion
ConclusionThis Danish population-based study found a high occurrence of patient-reported persisting symptoms following the acute phase of COVID-19 infection, which were associated with the discontinuation of immunosuppressive therapies for UC during COVID-19 and the severity of COVID-19 among patients with CD. These findings might have implications for planning the healthcare of patients with inflammatory bowel diseases in the post-COVID-19 era.
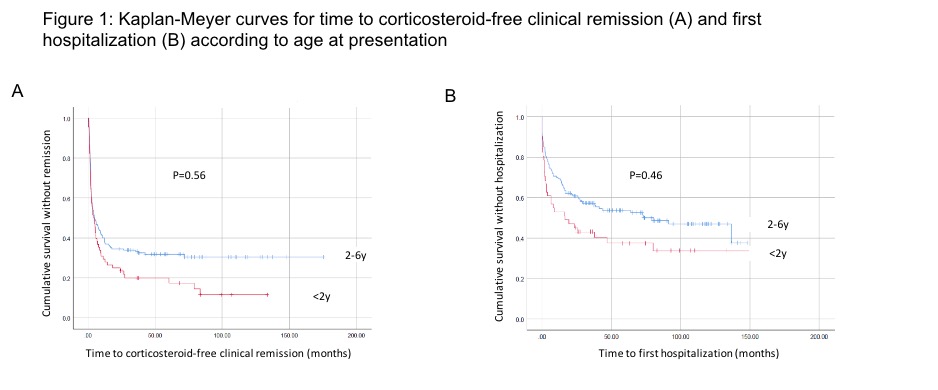
Very early-onset inflammatory bowel disease (VEOIBD) is diagnosed before the age of 6 years while infantile IBD occurs before the age of 2 years. We aimed to assess disease characteristics and long-term outcomes in these populations.
MethodsWe conducted a retrospective longitudinal cohort study in 21 pediatric centers worldwide. Patients diagnosed with VEOIBD between the years 2008-2018 with at least 2 years of follow-up were included.
ResultsThe cohort included 243 patients (52% males), with median follow-up of 5.8 (IQR 3.2-8.4) years. Median age at diagnosis was 3.3 (IQR 1.8-4.5) years, with 69 (28%) diagnosed before the age of 2 years. Disease was classified as Crohn’s disease (CD), ulcerative colitis (UC) and IBD-unclassified (IBDU) in 30%, 59% and 11%, respectively. In patients with UC or IBDU, 75% presented with pancolitis. In patients with CD, 62% presented with isolated colonic disease and 32% with ileo-colonic disease, while 19% had perianal involvement. Genetic testing was performed in 96 (40%) patients [40 (58%) <2 years, 56 (32%) 2-6 years, p=0.001], with monogenic diagnosis identified in 23% (33% and 16%, respectively, p=0.08). The most common findings were mutations in IL10-receptor (5 cases, 23%). Stricturing or penetrating disease was observed in 9 cases (4%).
First induction therapies were corticosteroids, 5-aminosalicylic acid (5ASA) and nutritional therapy in 53%, 30% and 11%, respectively. Corticosteroids were more common as first induction in infantile vs. non-infantile IBD (64% vs. 49% respectively, p=0.003). Maintenance therapies included deep immune-suppression (mainly biologics and corticosteroids) in 51%, immunomodulators in 27%, and non-immunosuppressive agents (5-ASA, nutritional therapy and antibiotics) in 22% of patients, with no significant differences between age groups.
Compared to patients diagnosed after 2 years of age, patients with infantile IBD presented with higher rates of IBDU, lower levels of hemoglobin and albumin and higher levels of CRP, lower weight (but not height) z-scores, had lower rates of response to first induction therapy and shorter time to hospitalization during follow-up (p<0.05 for all).
Colectomy was performed in 11% and diversion surgery in 4% of the cohort, with no significant differences between age groups. No malignancies and nor deaths were observed. At end of follow-up, 85% of patients were in corticosteroid free clinical remission.
 Conclusion
ConclusionPatients with VEOIBD, including infantile IBD, have fair long-term outcome with low rates of complications and surgical interventions. Nevertheless, patients with infantile IBD demonstrated more severe clinical features at presentation and a lower response to induction therapy.
In the UNIFI study of ustekinumab (UST) in ulcerative colitis (UC), patients who achieved histo-endoscopic mucosal healing (HEMH; ie, both histologic and endoscopic improvement of mucosa) after induction had higher clinical remission and corticosteroid-free clinical remission rates through 1 year than those who achieved either histologic or endoscopic improvement alone.1 Here, we report the effect of achieving HEMH after induction on long-term symptomatic outcomes through 3 years.
MethodsPatients who were in clinical response after 8 wks of IV induction with UST 130mg or ~6mg/kg (wk 8 responders) were randomized to maintenance treatment with SC UST 90mg q12w or q8w on entry into maintenance. Those who were not in clinical response to the initial UST dose at wk8 but achieved response at wk16 after receiving a single SC dose of UST 90mg at wk8 (wk16 responders) entered maintenance receiving SC 90mg q8w. After 44 wks of maintenance treatment, patients were given the option to continue in the long-term extension. HEMH was defined as achieving both endoscopic improvement (Mayo endoscopy subscore ≤1) and histologic improvement (neutrophil infiltration in <5% of crypts, no crypt destruction, and no erosions, ulcerations, or granulation tissue; based on the Geboes score). Patients with insufficient data for histologic evaluation at the end of induction were excluded. Symptomatic remission was defined as a Mayo stool frequency subscore of 0 or 1 and a Mayo rectal bleeding subscore of 0.
ResultsOf the 438 patients who were wk8 or wk16 responders to UST induction and received UST maintenance, 116 (26.5%) achieved HEMH after induction, 30 (6.8%) achieved endoscopic improvement without histologic improvement (EI), and 106 (24.2%) achieved histologic improvement without endoscopic improvement (HI). Patients who achieved HEMH after induction had higher symptomatic remission and corticosteroid-free symptomatic remission rates at wks92 and 152 than those with EI or HI; the differences were statistically significantly greater at wk152, while they were only numerically greater at wk92 (Table). The differences were primarily driven by patients with HEMH after induction being more likely to maintain symptomatic remission between wks92 and 152, than those with EI or HI alone. Symptomatic remission and corticosteroid-free remission rates decreased between wks92 and 152 in patients with EI or HI only.
Patients with UC who achieved HEMH after induction with UST were more likely to maintain symptomatic remission and corticosteroid-free symptomatic remission between 2 and 3 years of maintenance treatment than those who achieved EI or HI alone.
1. K Li, et al. Poster 1008. Presented at UEGW 2019. October 22, 2019. Barcelona, Spain.
Ozanimod was approved by the FDA to treat patients (pts) with moderately to severely active Ulcerative Colitis (UC) based on the results from the 52-week (wk) phase 3 True North (TN) study. We sought to evaluate long-term efficacy and safety of ozanimod.
MethodsWe examined data from an interim analysis of pts in the TN parent study who entered the ongoing TN open-label extension (OLE). Pts entered the TN OLE from the phase 3 TN study if they were non-responders at the end of induction, lost response during maintenance, or completed maintenance treatment, or from the phase 2 Touchstone OLE if they remained at study closure and received once-daily oral ozanimod 0.92 mg (equivalent to ozanimod HCl 1 mg). Clinical remission, clinical response, endoscopic improvement, and corticosteroid (CS)-free remission were evaluated at Wks 46, 94, and 142 in the TN OLE for all pts who entered the OLE from the TN parent study, and in the subset of pts in clinical response at the OLE entry. The data were analysed in the intent-to-treat population using observed cases (OC), which used the number of pts remaining in the study at the corresponding time point, and non-responder imputation (NRI), which used the number of pts remaining in the study at the corresponding time point and those who withdrew before the time point but would have reached the time point if they had stayed. Treatment-emergent adverse events were evaluated from the pooled phase 2 and phase 3 UC studies.
ResultsA total of 823 pts from TN entered the TN OLE; as of the cut-off date (Sept 30, 2020), 64% completed Wk 46, 34% completed Wk 94, and 14% completed Wk 142 of the OLE. The most common reason for discontinuation was lack of efficacy (21%). Baseline demographics were similar as in the TN study. A total of 261 pts were in clinical response at the time of OLE entry. OC analyses showed that the percentage of pts achieving clinical remission, clinical response, endoscopic improvement, and CS-free remission was maintained over time (Table). Efficacy in the responders was higher compared to the total population and was comparable within the endpoints at Wks 46 and 94. Using the more conservative NRI analysis, the proportion of pts achieving each endpoint was lower than in the OC; however, after 94 wks of OLE treatment, 34% of all pts and 55% of the responders still maintained clinical response. No new safety signals were seen with longer-term ozanimod use in the 1158 pts in the pooled population.
ConclusionUC pts from the phase 3 TN study demonstrated maintenance of response with long-term ozanimod treatment. These data reflect approximately 2 years of additional ozanimod treatment, with no new safety signals identified.