Exabis Library
Welcome to the e-CCO Library!
Abdominal pain (AP), bowel urgency (BU), and fatigue are debilitating symptoms that reduce quality of life in patients with active ulcerative colitis (UC). Results from two Phase 3 induction trials (U‑ACHIEVE induction [NCT02819635] and U‑ACCOMPLISH [NCT03653026]) showed significant improvements in AP, BU, and fatigue following induction with upadacitinib (UPA) in patients with active UC who had previously failed conventional or biologic therapy. We evaluated the effects of 52-week UPA maintenance treatment on AP, BU, and fatigue in patients who achieved a clinical response after induction.
MethodsFour hundred fifty-one patients who achieved a clinical response after 8 weeks of induction with UPA 45 mg once daily (QD) were enrolled in the U-ACHIEVE maintenance study and were re-randomised 1:1:1 to UPA 15 mg QD (n=148), UPA 30 mg QD (n=154), or placebo (PBO) QD (n=149). Endpoints in this analysis were the percentage of patients who reported no AP or no BU at Weeks 0, 4, 8, 20, 28, 36 and 52, respectively, and the change in Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT–F) from induction baseline to Weeks 0 and 52 in the maintenance study. Patients recorded AP and BU daily via an electronic, handheld device. Lastly, the percentage of patients reporting a clinically meaningful within person change (MWPC), defined as ≥5-point increase in FACIT-F score from induction baseline, and normalization of fatigue, defined as a FACIT-F score >40 points, were determined at Weeks 0 and 52.
ResultsSignificantly more patients reported no AP at Week 8 for UPA 15 mg vs PBO (60.8% vs 48.3%, p<0.05, Figure 1) and at Week 12 for UPA 30 mg vs PBO (59.7% vs 43.6%, p<0.01); significant differences were maintained through Week 52 (15 mg: 45.9%; 30 mg: 55.3% vs PBO: 20.8%, p<0.001). For no BU reported, significant differences vs PBO were observed with UPA 30 mg at Week 4 (68.8% vs 54.4%, p<0.05, Figure 2) and with UPA 15 mg at Week 8 (64.9% vs 49.7%, p<0.01) and were maintained through Week 52 (15 mg: 56.1%; 30 mg: 63.6% vs PBO: 17.4%, p<0.001). A significantly greater percentage of patients achieved MWPC in FACIT-F with both UPA 15 mg (55.4%) and UPA 30 mg (58.8%) compared with PBO (35.1%; p<0.001) at Week 52. In addition, a greater percentage of UPA-treated patients achieved normalization of fatigue (52.0% and 55.7% for UPA 15 mg and UPA 30 mg, respectively) vs PBO (35.7%) at Week 52 (p<0.01).
ConclusionIn patients with moderately to severely active UC who responded to UPA 45 mg induction treatment, significant and clinically meaningful improvements in patient-reported AP, BU, and fatigue achieved during induction were sustained through 52 weeks of UPA 15 mg or 30 mg maintenance treatment.


The QUASAR Induction Study 1 (NCT04033445) is a phase 2b randomized, double-blind, placebo-controlled, dose-ranging study to evaluate the efficacy and safety of guselkumab (GUS), an interleukin-23 p19 subunit antagonist, as induction therapy in patients with moderately to severely active ulcerative colitis (UC) who had an inadequate response or intolerance to conventional (ie, thiopurines or corticosteroids) or advanced therapy (ie, tumor necrosis factor alpha antagonists, vedolizumab, or tofacitinib).
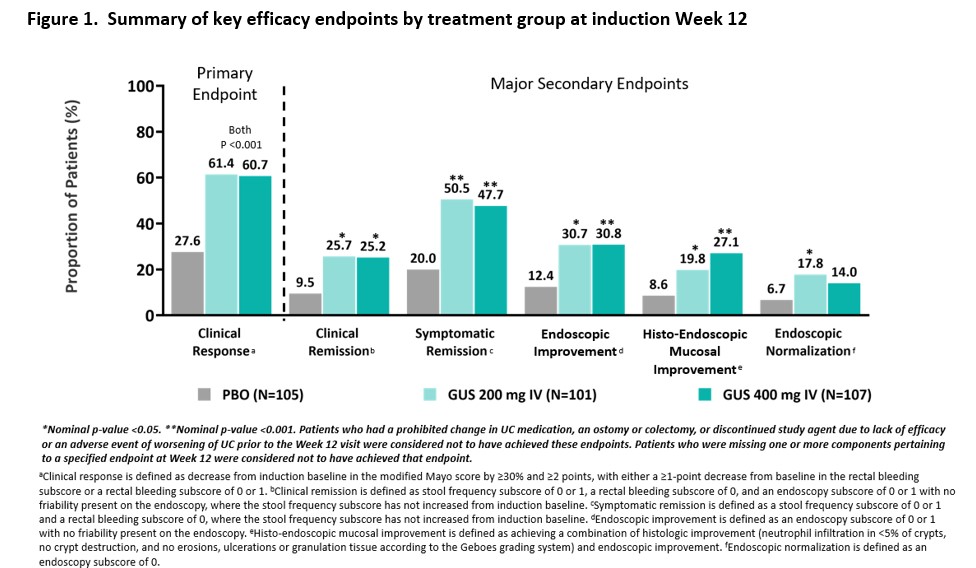
MethodsPatients included in these analyses had moderately to severely active UC (defined as a modified Mayo score of 5 to 9, inclusive) with a Mayo rectal bleeding subscore ≥ 1 and a Mayo endoscopy subscore ≥ 2 obtained during central review of video endoscopy at baseline. Patients were randomized 1:1:1 to receive IV GUS 200 mg, 400 mg, or placebo at Weeks 0, 4, and 8. The primary endpoint was clinical response at Week 12, and major secondary endpoints included clinical remission, symptomatic remission, endoscopic improvement, histo-endoscopic mucosal improvement, and endoscopic normalization at Week 12. Type 1 error was controlled at the 0.05 significance level for the primary endpoint; no other endpoints were controlled for multiplicity. Safety was assessed through Week 12.
ResultsThree hundred thirteen patients were randomized in the primary analysis population (mean age, 41.6 yrs; male 59.1%, mean UC duration, 7.55 yrs; mean Mayo score, 9.2; endoscopy subscore of 3 indicating severe disease, 70%; baseline oral corticosteroid use, 39.6%). Approximately 50% had a prior inadequate response or intolerance to advanced therapy for UC. The baseline demographics and disease characteristics were generally similar among treatment groups (Table 1). At Week 12, a significantly greater proportion of patients treated with GUS 200 mg and 400 mg achieved clinical response compared with placebo (61.4% and 60.7% vs 27.6%, respectively, both p<0.001). A greater proportion of GUS-treated patients compared with placebo-treated patients achieved the major secondary endpoints at Week 12 (Figure 1). The proportions of patients reporting adverse events, serious adverse events, and adverse events leading to discontinuation in the GUS groups were not greater compared with placebo (Table 2). No serious infections were reported for GUS. No cases of malignancy or death were reported.

 Conclusion
ConclusionIn patients with moderately to severely active UC, GUS induction treatment demonstrated superior efficacy compared with placebo treatment. Overall, safety results through Week 12 were consistent with the known safety profile of GUS in approved indications. The efficacy and safety of GUS 200 mg and 400 mg were comparable.
Background
Endoscopic and histologic activity are important therapeutic targets in ulcerative colitis (UC). The Paddington International Virtual ChromoendoScopy ScOre (VCE-PICaSSO)1 demonstrated that enhanced visualisation of subtle mucosal and vascular inflammatory changes correlated strongly with histology. However, without adequate training, the subjective evaluation of white light (WL) and VCE endoscopic scores varies between observers. We aimed to develop an artificial intelligence (AI) system for objective assessment of endoscopic disease activity and predict histology related to both white light and VCE videos.
MethodsMethods
469 endoscopy videos (48512 frames) from 235 patients representative of all grades of inflammation, from our prospective PICaSSO multicentre study1 were used to develop a convolutional neural network (CNN). 316 videos were divided into training (254) and validation (62) sets. 153 additional videos (78 patients) were used as test cohort. The videos were edited to separate clips with WL and with VCE, and assessed using Ulcerative Colitis Endoscopic Index of Severity (UCEIS) and PICaSSO, respectively. The classification stage of a pre-trained ResNet50 CNN classifier was trained to predict the healing or active inflammation on video frames. One network was trained to predict endoscopic remission (ER) as UCEIS≤1 from WL frames, and a second network was trained to predict PICaSSO≤3 from VCE. Histological remission (HR) was defined as Robarts Histological Index (RHI) ≤3 with no neutrophils in lamina propria or epithelium.
ResultsResults
In the validation cohort, our system predicted ER (UCEIS ≤1) in WL videos with 82% sensitivity (Se), 94% specificity (Sp) and an area under the ROC curve (AUROC) of 0.92. For the detection of remission in VCE videos (PICaSSO ≤3) Se was 74%, Sp 95%, and AUROC 0.95. In the testing cohort of independent videos, the diagnostic performance for both cut offs of ER remained similar. Table 1
Our system also had an excellent diagnostic performance for the prediction of HR in the validation set, with Se, Sp, and Accuracy of 92%, 83%, and 85% respectively, using VCE, and 83%, 87%, and 86% respectively, with WL. In the testing set performance declined modestly while remaining good. Of note, the algorithm’s prediction of histology was similar with VCE and WL videos. Table 2


Conclusions
Our AI system accurately recognize endoscopic remission in videos and predict histological remission equally well. This is the first AI model developed to analyse inflammation and endoscopic remission in VCE through the PICaSSO score, and the first multi-domain system providing a complete endoscopic and histologic assessment.
Reference
1. Iacucci et al. Gastroenterology 2021
IBD is a chronic immune-mediated disease that requires continuous patient care. The frequent contact and the good relationship with the multidisciplinary team (MDT) are essential for improving quality of life (QoL) and medication adherence aiming at treatment success. The aim of the study was to assess the importance of MDT in the view of patients with IBD and its impact on QoL and in medication adherence.
MethodsA cross-sectional study was carried out, including 114 patients from an IBD reference center in Brazil. The relevance of MDT was assessed through a questionnaire that included the importance of physicians, nurses, nutritionists and psychologists in the patient care. QoL was assessed by IBDQ. Treatment adherence and knowledge about the disease were assessed using the Morisky and CCKNOW questionnaires, respectively.
Results: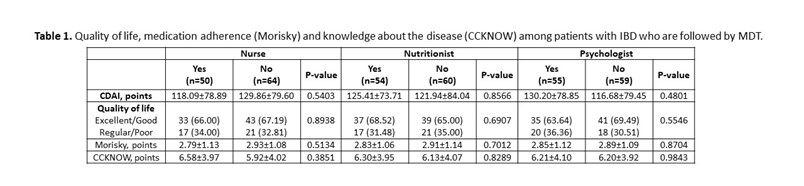 In total, 69 (60.53%) patients with CD and 45 (39.47%) patients with UC were included. The mean age was 39.16 (±13.50) years and 58.77% were female. The disease duration was 9.88 (±7.35) years. Presence of comorbidities was observed in 52.63% patients. About 57 (82.61%) patients with CD use biological therapy, with a statistical difference (p <0.0001) when compared to patients with UC (37.78%). The gastroenterologist was considered very important by 91.23% of patients, coloproctologist by 62.07% of patients, nurse by 65.05% of patients, nutritionist by 50% of patients and psychologist by 47.25% of patients. In the analysis of QoL, 24 (21.05%) patients had excellent QoL, 52 (45.61%) had good QoL, 29 (25.44%) had regular QoL and 9 (7.89%) had poor QoL, with no difference between patients who followed with nurses or other MDT professionals (Table 1). Medication adherence was low in 58.88% of patients. Knowledge about the disease was low (6.21 ± 3.99 points), being higher among patients with CD (p = 0.01). Patients identify the doctor as the main provider of care for their health, but about 10% leave with doubts from their appointments. 10% of patients think that more care with the nurse is necessary and less than 10% of patients are clarified by the nurse about QoL, ostomies, fecal incontinence, disease activity, biological therapy and sexuality.
In total, 69 (60.53%) patients with CD and 45 (39.47%) patients with UC were included. The mean age was 39.16 (±13.50) years and 58.77% were female. The disease duration was 9.88 (±7.35) years. Presence of comorbidities was observed in 52.63% patients. About 57 (82.61%) patients with CD use biological therapy, with a statistical difference (p <0.0001) when compared to patients with UC (37.78%). The gastroenterologist was considered very important by 91.23% of patients, coloproctologist by 62.07% of patients, nurse by 65.05% of patients, nutritionist by 50% of patients and psychologist by 47.25% of patients. In the analysis of QoL, 24 (21.05%) patients had excellent QoL, 52 (45.61%) had good QoL, 29 (25.44%) had regular QoL and 9 (7.89%) had poor QoL, with no difference between patients who followed with nurses or other MDT professionals (Table 1). Medication adherence was low in 58.88% of patients. Knowledge about the disease was low (6.21 ± 3.99 points), being higher among patients with CD (p = 0.01). Patients identify the doctor as the main provider of care for their health, but about 10% leave with doubts from their appointments. 10% of patients think that more care with the nurse is necessary and less than 10% of patients are clarified by the nurse about QoL, ostomies, fecal incontinence, disease activity, biological therapy and sexuality.
Patients considered doctors as the most important professionals in their care. Although the service has a multidisciplinary team, not all patients had the opportunity to consult with all professionals, mainly do the Covid pandemic in 2020 and 2021. The lack of contact with the entire team, especially with the nurse, may have contributed to low medication adherence and low knowledge of the disease, impacting disease control and QoL.