Exabis Library
Welcome to the e-CCO Library!
Fatigue is highly prevalent in patients with IBD independent of the disease status but treatment options remain limited. A potential mediator in the pathophysiology of fatigue is tryptophan (Trp), a precursor of serotonin. Recently, reduced serum Trp levels have been linked to fatigue in patients with clinically and endoscopically inactive IBD. The aim of the current study was to determine the effect of oral 5-hydroxytryptophan (5-HTP), the direct precursor of serotonin, supplementation on fatigue in patients with inactive IBD.
MethodsThis multicentre, randomized, double-blind, cross-over, placebo-controlled trial included fatigued patients with IBD in clinical and biochemical remission (CRP <10mg/L, calprotectin <250 mg/kg), treated with immunosuppressants and/or biologicals. Fatigue was assessed with the fatigue VAS (fVAS, range 0-10) and defined by a fVAS ≥5. Patients were treated in a cross-over manner with 100 mg 5-HTP or placebo bid for two consecutive periods of 8 weeks, without an intermediate washout period. The primary endpoint was the proportion of patients reaching a 20% reduction in fVAS after 8 weeks of intervention (week 8 versus week 0 and week 16 versus week 8). Secondary outcomes were changes in validated FACIT-F score, scores for depression and anxiety and changes in Trp metabolites. The effect of the intervention on the outcomes was evaluated by linear mixed modelling (LMM), with the intervention, period and intervention x period as fixed factors and study participant as random factor.
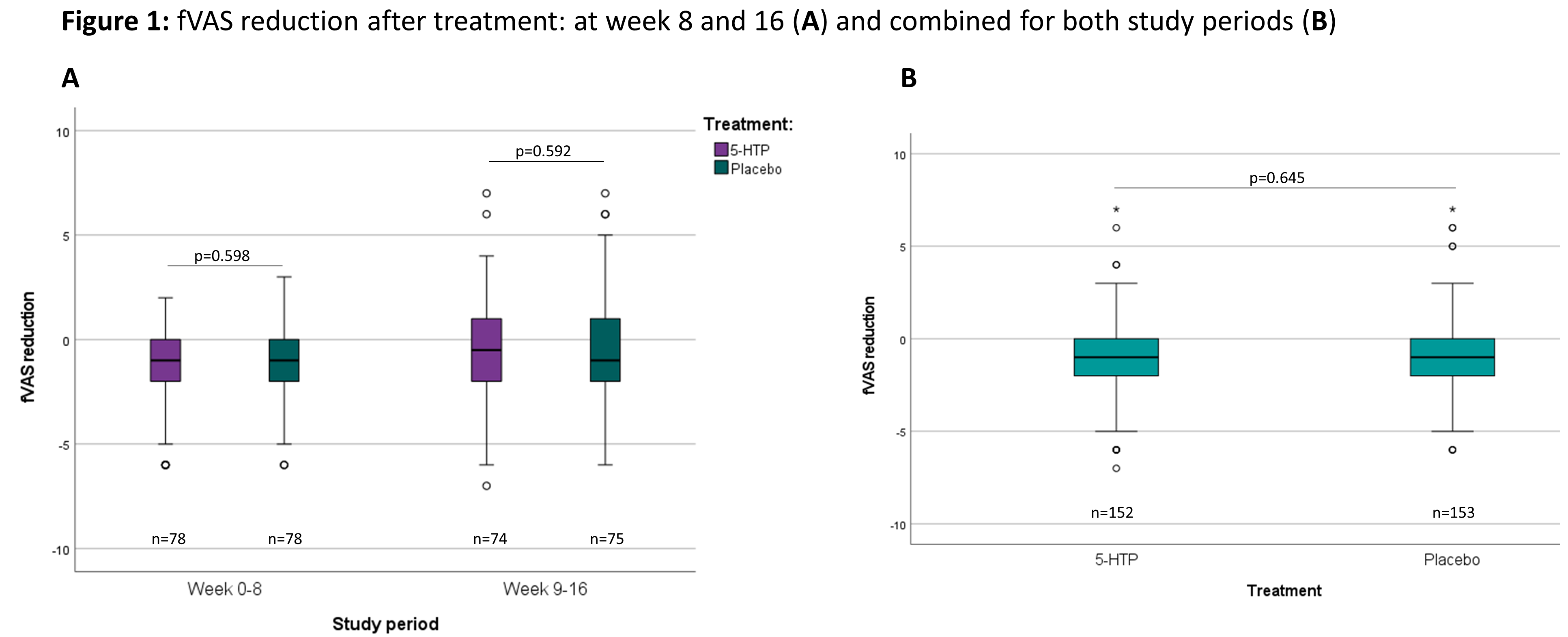
ResultsA total of 166 patients were included in 13 Belgian centres between December 2018 and November 2020 (baseline characteristics: Table 1). The dropout rate was 10.8%. The evolution of the fVAS throughout the study was comparable between both study groups and no difference was observed in fVAS reduction between placebo and 5-HTP (Figure 1). The proportion of patients reaching ≥20% reduction in fVAS did not differ between placebo (37.6%) and 5-HTP (35.6%) (p=0.830). The evolution of the other scores for fatigue, depression, anxiety and stress were also similar between placebo and 5-HTP (Table 2). A significant increase in 5-HTP and serotonin serum levels was observed during 5-HTP treatment compared to placebo; whereas serum levels of Trp and kynurenine were comparable. Globally, changes in fVAS were not associated with changes in those metabolites (Figure 2). Adverse events (AEs) were seen in 29.2% and 34.8% of patients under treatment with placebo and 5-HTP respectively (p=0.282).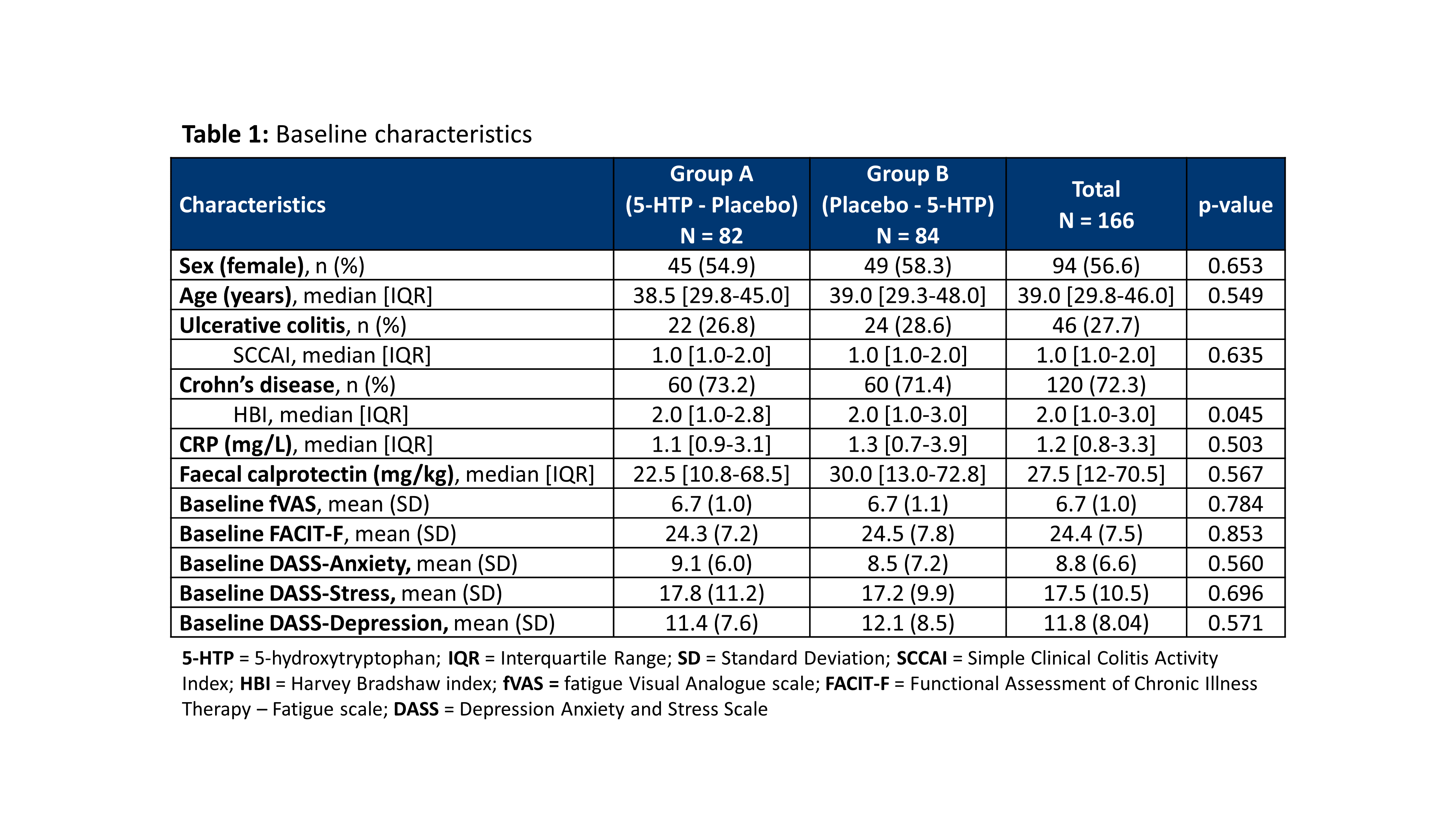


Despite a significant increase in serum 5-HTP and serotonin levels by oral treatment with 5-HTP, 5-HTP did not modulate IBD-related fatigue. Furthermore, treatment with 5-HTP had no impact on depression, anxiety and stress scores.
Accurately predicting disease course at diagnosis is critical to facilitate personalized therapy in inflammatory bowel disease (IBD). PredictSURE IBDTM is a whole blood qPCR assay that was developed to predict prognosis in newly diagnosed, treatment-naïve IBD patients – classifying them into IBDhi (high-risk) or IBDlo (low-risk). The current recommendation is that PredictSURE IBDTM should not be used in those who have commenced steroids. In this study, we aimed to determine the impact of steroid therapy on the performance of PredictSURE IBDTM .
MethodsWhole blood was serially taken from patients admitted with severe IBD requiring intravenous (IV) steroids (pre-steroid, day 3, day 5; n=10, cohort 1) and from patients receiving oral steroids as outpatients (pre-steroid, week 1, week 6; n=10, cohort 2). An independent cohort of 43 IBD patients, all within 3 months of diagnosis and on corticosteroid treatment (41 systemic and 2 topical, cohort 3) was recruited. RNA was extracted and analyzed with PredictSURE IBDTM (PredictImmune, UK). Patients were prospectively followed and treated according to routine clinical management by physicians blinded to the test results, and clinically stratified according to one of the original definitions used to construct and validate the test (need for step up to immunosuppressive or biological therapy or surgery).
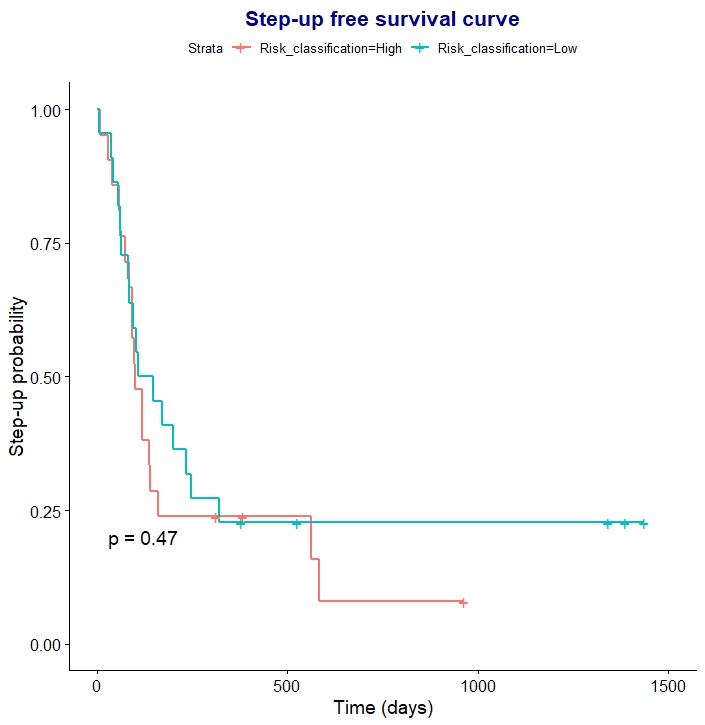
ResultsIn cohorts 1 and 2, both oral and intravenous steroids affected the PredictSURE IBDTM result: misclassification as IBDlo occurred in 5/8 IBDhi patients receiving oral, and 5/7 IBDhi patients receiving IV, steroids. In 60% this change was detectable early (within 1 week of oral steroids and 3 days of IV steroids). Steroids did not affect the classification of IBDlo patients. Consistently, the prognostic accuracy was limited in patients already receiving steroids (cohort 3). After a median follow-up of 31.8 [IQR 18.7 - 42.1] months, 35 (81%) patients required step-up therapy. PredictSure IBDTM correctly classified only 23 (54%) patients with accuracy of 0.53 (sensitivity: 0.51, specificity: 0.63, positive likelihood ratio: 1.38, negative likelihood ratio: 0.77). Seventeen (80%) of the misclassifications were clinically high-risk patients who were predicted as IBDlo. Time to treatment escalation was similar between patients classified as IBDhi or IBDlo after starting steroid therapy (p= 0.47) (Figure 1).
The prognostic accuracy of PredictSURE IBDTM is limited if performed after steroid therapy has begun, most likely because of the misclassification of high-risk patients as low risk. Therefore, the test should only be performed in patients with active disease who are not receiving steroid therapy, as currently recommended.
Measuring food-related quality of life (FRQoL) quantifies the psychosocial impact of eating and drinking.1 The influences on FRQoL in people with inflammatory bowel disease (IBD) are not well explored, despite IBD being a chronic disease affecting the digestive tract. This study aimed to characterise and identify any patient or disease-related predictors of FRQoL in individuals with IBD.
MethodsAdults with a formal diagnosis of IBD were recruited to a prospective multi-centre cross-sectional study between April 2018 and December 2019. Participants completed questionnaires measuring FRQoL (IBD-FRQoL-29: minimum/poor 29, maximum/greatest 145), clinical disease activity (active disease: Harvey Bradshaw Index >4 active disease, Simple Clinical Colitis Activity Index >2, restrictive eating behaviour (Nine Item Avoidant/Restrictive Screen: minimum 0, maximum 45), mental health (DASS-21: minimum 0, maximum 126) and other patient and disease-related variables.
ResultsOne hundred and eight participants completed the questionnaires. The majority of the cohort had UC (69/108, 64%) and there was almost equal distribution of those with quiescent (48%) and active (52%) disease The mean FRQoL of individuals with IBD was 79 (95% CI 75, 84) (see Figure 1). Poorer FRQoL was seen in those with restrictive eating behaviour associated with fear of a negative consequence from eating (p<0.0001) and reduced appetite (p<0.030). Greater FRQoL was seen in those with lower disease activity (p<0.0001) and previous IBD surgery (p=0.240). FRQoL was not influenced either way by IBD phenotype, duration, or gender. The majority of participants obtained their dietary information from the internet (60%) or gastroenterologist (46%).
FRQoL in people with IBD is poorer in those with restrictive eating behaviours and clinically active disease. Interestingly, it was greater in those with previous IBD surgery. Further research is required to validate these associations and explore longitudinal effects of poor FRQoL on patient outcomes and potential strategies for prevention or management of impaired FRQoL in IBD.
References
1Hughes LD, King L, Morgan M, et al. Food-related quality of life in inflammatory bowel disease: Development and validation of a questionnaire. J Crohns Colitis 2016;10:194-201.
Recent progress in deciphering the complex pathogenesis of Crohn’s disease (CD) has yielded several effective biologicals. However, ambitious therapeutic goals remain unfulfilled as almost 30% of patients are primary non-responders to a particular biological. This underscores the need for easy-to-implement biomarkers that predict (non-)remission. We aimed to identify serum protein biomarkers that predict endoscopic remission in CD patients.
MethodsSerum samples from 169 consecutive CD patients with active endoscopic disease (presence of ulcerations) before starting a biological [infliximab (IFX), adalimumab (ADA), vedolizumab (VDZ) or ustekinumab (UST)] to which they were naïve were collected. Patients were prospectively followed with endoscopic re-assessment after 6-12 months. There were 102 patients (Table 1) with endoscopic remission (SES ≤ 2 or disappearance of all ulcers), whereas 67 showed no improvement. Two independent and complementary proteomic platforms were used: 644 proteins belonging to predesigned assays were quantified using Proximity Extension Assay (PEA) technology (Olink Proteomics AB, Sweden). Second, wide protein discovery mass spectrometry (MS)-based technic (Caprion, Canada) was used and quantified another 985 proteins. A multivariate modelling framework was then applied on a randomly selected training sub-cohort (85%). Predictive performance of identified panels was assessed on the remaining test sub-cohort (15%). We sought to implement the same framework on the drug-specific subgroups; however, train/test splitting was not possible in IFX or ADA subgroups due to very few observations in the non-remission arms which diminishes the possibility for reliable predictive modelling.

Applying the modelling framework on training sets from the general cohort, VDZ subgroup and UST subgroup, proteomic panels were selected and consisted of 26, 6 and 8 proteins, respectively, and showed high performance in the test sets (Table 2). VDZ and UST panels shared only 2 proteins each with the general panel, and had no predictive power (accuracy ≤ 0.5) when used to predict other subgroups, making them specific to their respective drugs. Selected proteins are involved among others in pro-inflammatory, extracellular matrix modelling, coagulation and cellular-vascular interaction pathways (Table 3).


Applying a multivariate machine learning algorithm on a wide pool of serum proteomics analysed through two discovery technics, we were able to identify 3 proteomic panels that can predict endoscopic (non)remission in patients with CD. Exact implication of these proteins in intestinal inflammation and a validation in an independent cohort is being further investigated.
Ulcerative Colitis (UC) associated single nucleotide polymorphisms (SNP) are mostly in non-coding regions of the genome. Because of that, it has been challenging to determine their role in the disease onset and severity. We have previously developed an integrative workflow (termed iSNP) to understand better how these SNPs are involved in the pathogenesis of UC. Here we present a recent update both in the methodology and new results, including a new player for prediction of therapeutic escalation in UC.
MethodsFrom immunochip data of 376 UC patients of an East-Anglian, UK cohort, the SNPs were filtered for only the UC-associated ones. Then we predicted the SNPs’ effect on regulatory interactions using two complementary transcription factor-target gene prediction methods, RSAT and FIMO. SNPs were considered if the SNP was located in the promoter region of a gene or in an enhancer region of a gene defined by the HEDD database. We considered a gene ‘SNP-affected’ if the risk allele and the non-risk allele had different transcription factor binding sites detected by any of the two methods. The proteins encoded by the SNP-affected genes were mapped to the integrated and high-confidence signaling network resource OmniPath. We also identified the direct physical interactors (first-neighbours) of these SNP affected genes/proteins. We created networks for each patient separately using their individual SNP-profiles. Finally, based on these patient-specific networks, we clustered patients in an unsupervised manner.
ResultsWe found 15 UC-associated SNPs which affected transcription factor binding sites, which in turn were modulating 54 genes. From these 54 SNP affected genes, 29 coded proteins that were present in the OmniPath signaling network. The patients formed five clusters, which were significantly correlated with therapeutic escalation defined by mesalazine or other more advanced therapy (p <0.05). Patients requiring immunomodulatory treatment have a greater prevalence of SNP RS943072 (G), corresponding to the transcriptional regulation of VEGF (vascular endothelial growth factor). VEGF is elevated in UC and stimulates angiogenesis, which is involved both in tissue regeneration and inflammation. VEGF is upregulated in the presence of this risk SNP causing increased inflammatory phenotype.
We updated the iSNP method by including enhancer regions and multiple transcription factor binding site prediction methods, and were able to predict that those UC patients who have a VEGF-affecting SNP require therapeutic upscaling.
The efficacy and safety of risankizumab (RZB) as induction and maintenance therapy forpatients with moderately to severely active Crohn’s disease (CD) has been documented. Steroid-free clinical remission is an important additional treatment goal in CD. The efficacy of RZB by baseline steroid use during induction and steroid-free outcomes during maintenance was examined.
MethodsIn ADVANCE (NCT03105128) and MOTIVATE (NCT03104413), patients with moderately to severely active CD received intravenous (IV) RZB induction therapy or placebo (PBO) for 12 weeks. Patients with clinical response to RZB were re-randomised in a 52-week maintenance study (FORTIFY; NCT03105102) to subcutaneous (SC) RZB or PBO (ie, withdrawal). Patients receiving steroids (maximum prednisone or equivalent ≤ 20 mg/day; budesonide ≤ 9 mg/day) at baseline of the induction studies maintained stable doses for the 12-week study duration. A mandatory steroid taper per protocol was initiated at the beginning of maintenance for patients receiving steroids during induction. Patients losing clinical response (per investigator assessment) after initiation of taper could have their steroid dose increased up to the induction baseline dose. This analysis included patients who received RZB 600 mg IV in ADVANCE or MOTIVATE and patients who received RZB 360 mg SC in FORTIFY. Endpoints reported included clinical remission (defined by CD Activity Index [CDAI] or stool frequency/abdominal pain score [SF/APS] criteria) at week 12 of induction by baseline steroid use, steroid-free clinical remission (CDAI or SF/APS), steroid-free endoscopic response, and steroid-free endoscopic remission at week 52 of maintenance. Steroid discontinuation rates over 52 weeks of maintenance were also assessed.
ResultsInduction of clinical remission at week 12 with RZB 600 mg IV in ADVANCE or MOTIVATE was independent from baseline steroid use (Figure 1).Clinical remission rates (CDAI or SF/APS) at week 12 were similar for patients using steroids vs those who were not (33.8%–42.0% vs 34.9%–46.6%; Figure 1). Steroid use decreased over time in FORTIFY, with a greater proportion of patients receiving RZB 360 mg SC discontinuing steroids at week 52 vs withdrawal (PBO SC; Figure 2A). Rates of steroid-free clinical remission (P ≤ .012), steroid-free endoscopic response (P < .001), and steroid-free endoscopic remission (P < .001) were significantly higher with RZB 360 mg SC vs withdrawal (PBO SC) at week 52 of maintenance (Figure 2B–2C).

Efficacy of RZB induction therapy was independent of baseline steroid use. RZB maintenance promotes high rates of steroid-free clinical and endoscopic outcomes, demonstrating a benefit of RZB treatment in CD.