Exabis Library
Welcome to the e-CCO Library!
Robust and sensitive therapeutic targets are key in effective management of Inflammatory Bowel Disease1. Mesenteric hyperaemia is a recognized sign of active disease and in cross-sectional image is described as the comb sign. Although it is subjectively described, no automated quantitative MRI-based measures have been developed.
We aim to develop an automated methodology using contrast-less time of flight (TOF) Magnetic resonance angiography (MRA).
MethodsA MATLAB algorithm was developed to track the vessels on a 3D maximum intensity projection of a TOF MRA data set and calculate an arborization Index which is the number of branching points in the intrabdominal vessels (figure 1). 2D TOF scans were acquired in the transverse plane between the top of the hip joint and L4 vertebra using a 3T Ingenia Wide bore scanner (Philips, The Netherlands). The primary outcome was a comparison of the arborization index between Crohn’s disease (CD) and healthy volunteers (HV) groups. A planned sub-analysis was undertaken across CD and HV matched for BMI to investigate the effect of visceral fat on the arborization index. Repeated measures were undertaken to evaluate the variability of the quantification method. No contrast agents were used for the TOF MRA scans. Biological variations within each group and test-retest repeatability were assessed using the coefficient of variation (CV). Statistical analysis with unpaired, two-tailed t-tests were conducted and differences were considered significant when the p-value ≤0.05. All absolute values are presented as mean ±standard deviation (SD).
In this prospective pilot study, 7 CD patients (C-Reactive Protein=5.2±6.1 mg/L, Faecal Calprotectin 611±981μg/g, BMI=23±3 kg/m2) and 15 HVs (BMI=29±7 kg/m2) were recruited. Patients showed a significantly higher arborization index when compared to HVs (mean arborization in HV=94±21 and CD=139±26; p-value=0.002). The difference in arborization index persisted in a sub-analysis of 7 HVs (BMI=24±2 kg/m2) and 7 CD patients (mean arborization in matched HVs=101±22 vs mean index in CD=139±26; p=0.01) (Figure 2). The CV was 23% for HVs and 18% for CD indicating biological variation. Test-retest variability calculated from multiple TOF scans of the same subjects gave a mean CV of 6±5% for both groups combined.
Our preliminary data suggest that the arborization index may be a useful measure of hypervascularity and hence intestinal inflammation in Inflammatory Bowel Disease. Further validation to standard disease activity measures is needed across larger cohorts to better investigate the utility of this potential biomarker as a non-invasive measure of disease activity and its reversibility to IBD therapies.
1.Turner,D.,et al.Gastro.2021;160(5):1570-1583.
To clarify the risk of lymphoma in patients with inflammatory bowel diseases (IBD) exposed to anti-tumor necrosis factor (anti-TNF) and/or thiopurines we aimed to evaluate the Israeli IBD population.
MethodsA nested case-control study on the epidemiology cohort of the Israeli IBD Research Nucleus (epi-IIRN) including all 4 Health Maintenance Organizations in Israel linked to the Israeli Cancer Registry. Patients diagnosed since 1.1.2005 until 31.12.2015 (42,954 patients) were included and followed until 31.12.2017. Each lymphoma case was matched to 30 non-lymphoma IBD patients by age, gender, IBD subtype, and date of earliest evidence of IBD in the database. Patients with other risk factors for lymphoma, or lymphoma diagnosis prior to IBD diagnosis were excluded (figure 1). Conditional logistic regression was used to compute the association of drug exposure (anti-TNF, thiopurines and combination) with diagnosis of lymphoma. Patients without exposure to anti-TNF and/or thiopurines in each group served as reference within each group. Additionally, sub-group analyses by gender, age group at inclusion (≤48, 49-64, ≥65), time from last drug exposure (≤90 days, 91-365 days, >365 days) were done.
The final nested cohort included 5556 IBD patients (185 lymphoma cases matched to 5,371 without lymphoma). Mean follow-up (F/U): 5.5±3.5 years, 50% with Crohn’s disease, mean age at database entry 52.6±17.80 years. Anti-TNF-only exposure was documented in 4.3% (8/185) of lymphoma cases vs. 2.6% (145/5,371) of controls OR 1.97, CI 0.93-4.16, p=0.07; in males the ORs were 2.84 (CI 1.17-6.92 p=0.04) and increased to OR 3.48 (CI 1.55-7.88, p=0.002) for males <48 years and OR 2.87 (CI 1.53-5.37, p=0.001) for patients with last exposure ≤90 days (figure 2). Exposure to combination anti-TNF+thiopurines occurred in 8.6% (16/185) of lymphoma cases vs. 5.3% (282/5,371) of controls OR 2.09 (CI 1.17-3.73, p=0.013). Males on anti-TNF-thiopurine combination had OR of 3.42 (CI 1.37-8.52, p=0.003) and in sequential (non-overlapping exposure to both thiopurines and anti-TNFs during F/U) combination an OR of 2.74 (CI 1.02-7.35 p=0.02). Thiopurine-only exposure occurred in 15.1% (28/185) of lymphoma cases vs. 13.5% (726/5,371) of controls, OR 1.32 (CI 0.86-2.03, p=0.20). Males on thiopurines had an OR of 1.75 (CI 1.02-2.99, p=0.05). The risk increased further in males <48 years OR 2.17 (CI 1.01-4.66, p=0.047) and in males aged≥65 OR 3.50 (CI 1.55-7.82, p=0.002). Females were not at risk for lymphoma (figure 3).

This nationwide study suggests that exposure to anti-TNF therapy alone or in combination with thiopurines may be associated with an increased risk of lymphoma, but only in males, especially when last exposure occurred within 90 days.
Breastmilk (BM) is a complex fluid that contributes to shaping the immune system of the offspring. BM composition depends on stage of lactation, maternal health status and diet, environment, and genetics. Limited data exists on the composition of the BM from women with IBD and its potential impact on the newborn’s microbiome composition.
MethodsThe MECONIUM (Exploring MEChanisms Of disease traNsmission In Utero through the Microbiome) study is a prospective cohort study including pregnant women with IBD, pregnant healthy control (HC), and their offspring. BM samples were collected 2 weeks post-delivery. Stool samples from the offspring were collected throughout the first 3 years of life and used to assess faecal calprotectin (fCal) and gut microbiota composition (16S). Targeted proteomics of the BM samples was performed with the Olink inflammation panel (92 protein biomarkers). Correlations between specific proteins in the BM, fCal and 16S were assessed using non-parametric tests. Multiple testing correction was performed with false discovery rate (FDR). MaAsLin2 R package was used for multivariate testing.
Results236 BM samples were analysed: 174 from HC, 37 Crohn’s disease (CD), 25 ulcerative colitis (UC). Thymic stromal lymphopoietin (TSLP), a cytokine with an important role in the maturation of T cells, was significantly lower in BM of women with IBD vs HC (FDR p=0.0017). The levels of TSLP in the BM of the mothers correlated negatively with infant fCal at year1 (rho=-0.20, p=0.01), and with the relative abundance of Cronobacter (MaAsLin2 FDR 0.1) of the offspring at month 1. Chemokine (C-C motif) ligand 20 (CCL20), which acts in chemotaxis of dendritic cells and T-cells and B-cells, was also significantly lower in women with CD vs HC (FDR 0.013) and in women with CD vs UC (p=0.014). Matrix metalloproteinase-1 (MMP-1), a collagenase involved in the breakdown of extracellular matrix, was also lower in BM of women with CD (p=0.009) and a negative correlation was observed between the levels of MMP1 and fCal at 3 months and 1 year (rho=-0.20 and -0.18, p=0.01 and 0.02, respectively). Osteoprotegerin (OPG), higher in BM of women with UC (p=0.018), was positively correlated with Streptococcus (MaAsLin2 FDR p=0.2) and negatively correlated with Bacteroides and Parabacteroides (MaAsLin2 FDR p=0.03 and 0.1) in the offspring at month 1.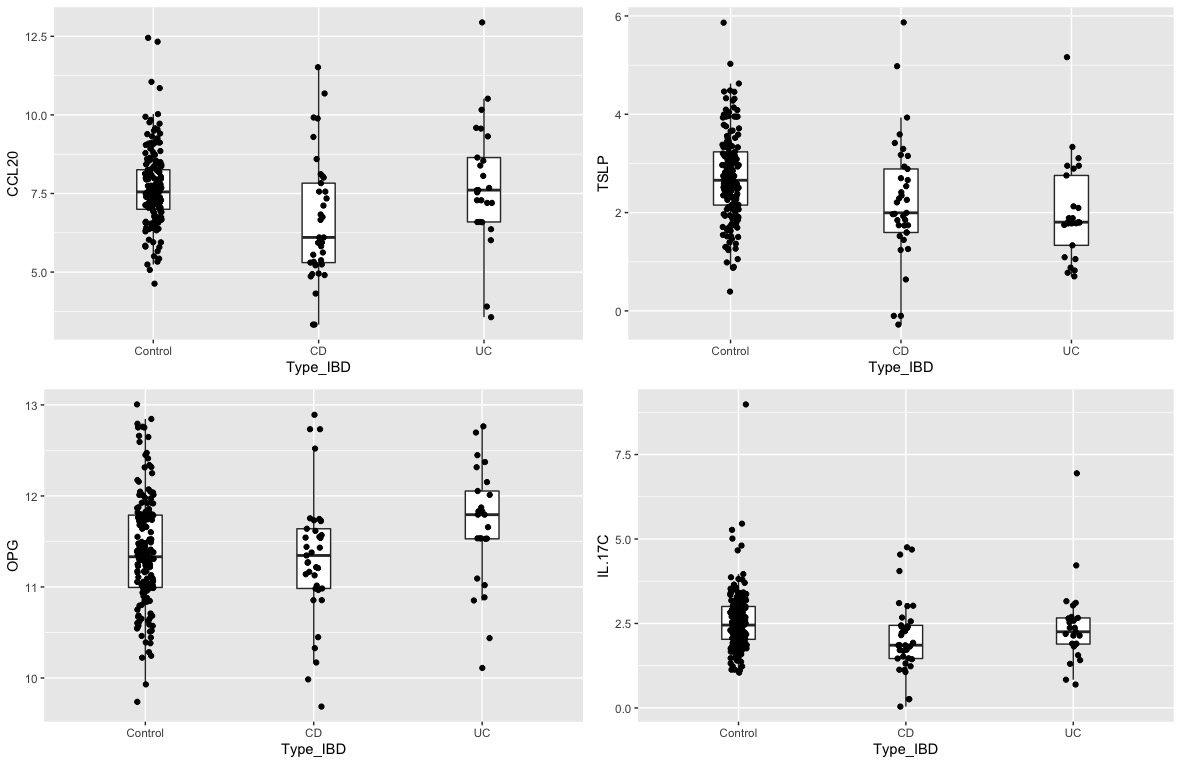
The proteomic profile of BM of women with IBD is distinct from that of women without IBD. BM composition may influence offspring’s’ gut microbiome signatures and fCal level at different timepoints. These findings suggest that BM composition may impact the offspring’s intestinal immune system maturation and microbiome development, and warrant further research.
Abdominal pain (AP), bowel urgency (BU), and fatigue are debilitating symptoms that reduce quality of life in patients with active ulcerative colitis (UC). Results from two Phase 3 induction trials (U‑ACHIEVE induction [NCT02819635] and U‑ACCOMPLISH [NCT03653026]) showed significant improvements in AP, BU, and fatigue following induction with upadacitinib (UPA) in patients with active UC who had previously failed conventional or biologic therapy. We evaluated the effects of 52-week UPA maintenance treatment on AP, BU, and fatigue in patients who achieved a clinical response after induction.
MethodsFour hundred fifty-one patients who achieved a clinical response after 8 weeks of induction with UPA 45 mg once daily (QD) were enrolled in the U-ACHIEVE maintenance study and were re-randomised 1:1:1 to UPA 15 mg QD (n=148), UPA 30 mg QD (n=154), or placebo (PBO) QD (n=149). Endpoints in this analysis were the percentage of patients who reported no AP or no BU at Weeks 0, 4, 8, 20, 28, 36 and 52, respectively, and the change in Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT–F) from induction baseline to Weeks 0 and 52 in the maintenance study. Patients recorded AP and BU daily via an electronic, handheld device. Lastly, the percentage of patients reporting a clinically meaningful within person change (MWPC), defined as ≥5-point increase in FACIT-F score from induction baseline, and normalization of fatigue, defined as a FACIT-F score >40 points, were determined at Weeks 0 and 52.
ResultsSignificantly more patients reported no AP at Week 8 for UPA 15 mg vs PBO (60.8% vs 48.3%, p<0.05, Figure 1) and at Week 12 for UPA 30 mg vs PBO (59.7% vs 43.6%, p<0.01); significant differences were maintained through Week 52 (15 mg: 45.9%; 30 mg: 55.3% vs PBO: 20.8%, p<0.001). For no BU reported, significant differences vs PBO were observed with UPA 30 mg at Week 4 (68.8% vs 54.4%, p<0.05, Figure 2) and with UPA 15 mg at Week 8 (64.9% vs 49.7%, p<0.01) and were maintained through Week 52 (15 mg: 56.1%; 30 mg: 63.6% vs PBO: 17.4%, p<0.001). A significantly greater percentage of patients achieved MWPC in FACIT-F with both UPA 15 mg (55.4%) and UPA 30 mg (58.8%) compared with PBO (35.1%; p<0.001) at Week 52. In addition, a greater percentage of UPA-treated patients achieved normalization of fatigue (52.0% and 55.7% for UPA 15 mg and UPA 30 mg, respectively) vs PBO (35.7%) at Week 52 (p<0.01).
ConclusionIn patients with moderately to severely active UC who responded to UPA 45 mg induction treatment, significant and clinically meaningful improvements in patient-reported AP, BU, and fatigue achieved during induction were sustained through 52 weeks of UPA 15 mg or 30 mg maintenance treatment.


The QUASAR Induction Study 1 (NCT04033445) is a phase 2b randomized, double-blind, placebo-controlled, dose-ranging study to evaluate the efficacy and safety of guselkumab (GUS), an interleukin-23 p19 subunit antagonist, as induction therapy in patients with moderately to severely active ulcerative colitis (UC) who had an inadequate response or intolerance to conventional (ie, thiopurines or corticosteroids) or advanced therapy (ie, tumor necrosis factor alpha antagonists, vedolizumab, or tofacitinib).
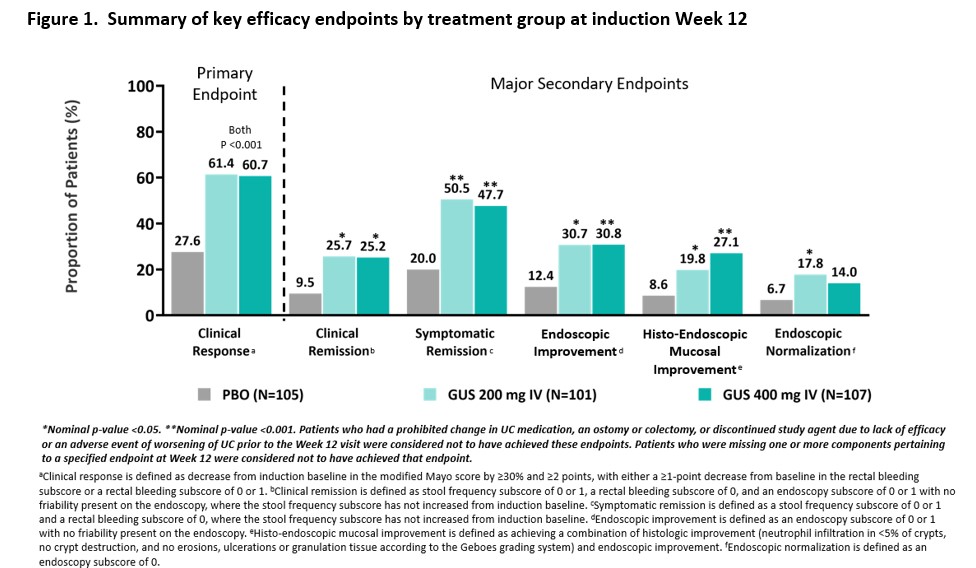
MethodsPatients included in these analyses had moderately to severely active UC (defined as a modified Mayo score of 5 to 9, inclusive) with a Mayo rectal bleeding subscore ≥ 1 and a Mayo endoscopy subscore ≥ 2 obtained during central review of video endoscopy at baseline. Patients were randomized 1:1:1 to receive IV GUS 200 mg, 400 mg, or placebo at Weeks 0, 4, and 8. The primary endpoint was clinical response at Week 12, and major secondary endpoints included clinical remission, symptomatic remission, endoscopic improvement, histo-endoscopic mucosal improvement, and endoscopic normalization at Week 12. Type 1 error was controlled at the 0.05 significance level for the primary endpoint; no other endpoints were controlled for multiplicity. Safety was assessed through Week 12.
ResultsThree hundred thirteen patients were randomized in the primary analysis population (mean age, 41.6 yrs; male 59.1%, mean UC duration, 7.55 yrs; mean Mayo score, 9.2; endoscopy subscore of 3 indicating severe disease, 70%; baseline oral corticosteroid use, 39.6%). Approximately 50% had a prior inadequate response or intolerance to advanced therapy for UC. The baseline demographics and disease characteristics were generally similar among treatment groups (Table 1). At Week 12, a significantly greater proportion of patients treated with GUS 200 mg and 400 mg achieved clinical response compared with placebo (61.4% and 60.7% vs 27.6%, respectively, both p<0.001). A greater proportion of GUS-treated patients compared with placebo-treated patients achieved the major secondary endpoints at Week 12 (Figure 1). The proportions of patients reporting adverse events, serious adverse events, and adverse events leading to discontinuation in the GUS groups were not greater compared with placebo (Table 2). No serious infections were reported for GUS. No cases of malignancy or death were reported.

 Conclusion
ConclusionIn patients with moderately to severely active UC, GUS induction treatment demonstrated superior efficacy compared with placebo treatment. Overall, safety results through Week 12 were consistent with the known safety profile of GUS in approved indications. The efficacy and safety of GUS 200 mg and 400 mg were comparable.