Exabis Library
Welcome to the e-CCO Library!
Ustekinumab (UST) and vedolizumab (VDZ) are widely used to treat patients with Crohn’s disease (CD). However, limited data exist regarding comparative effectiveness of these agents for patients with CD who have failed anti-TNF treatment. We aimed to compare the efficacy of UST and VDZ utilizing the largest cohort of CD patients who failed anti-TNF in real world clinical practice.
MethodsWe conducted a retrospective cohort analysis using data retrieved from the UK IBD BioResource, capturing 34,148 subjects. We identified patients with CD, who failed anti-TNF and were subsequently treated with UST or VDZ as second or third-line therapy. Inverse probability of treatment weighting (IPTW) was used to balance groups using a propensity score-weighting approach accounting for baseline patient or disease related characteristics. Persistence on therapy with clinician assessment of treatment success, without the need for treatment change or surgery was used to estimate the response to treatment. We compared treatment survival curves before and after IPTW and used a log rank test for differences between groups
Results654 CD patients received VDZ, either as second line (51%) or third line (49%) therapy. 365 patients received UST, 52% as a second line and 48% as a third line therapy. All patients received either infliximab or adalimumab as first and/or second biologic therapy. Baseline characteristics are detailed in table 1. Following IPTW, variables were well balanced. Patients receiving VDZ showed similar rates of treatment success compared to UST as second- and third-line biologic agent after anti TNF failure (before IPTW adjustment, log rank p 0.241; after IPTW, log rank p 0.154). Outcomes for UST were similar between 2nd and 3rd line usage (p 0.81), but outcomes for VDZ were significantly worse when used 3rd line compared to 2nd line (p <0.0001).Subgroup analysis of unadjusted survival data showed significantly better outcomes for patients with ileal disease distributiontreated with UST compared to VDZ (p=0.043) but no significant differences in outcomes for subgroups with colonic or ileocolonic disease.We estimate persistence on UST and VDZ to be 67%, 54%, 49% and 49% at 1, 2, 3 and 5 years respectively.
ConclusionUsing data from a multi-institutional cohort of patients with CD with larger number of participants and longer follow-up than previous cohorts, we demonstrate no difference between UST and VDZ used as second and/or third line biologic therapy, after anti-TNF failure. Subgroup analysis reveals some patient characteristics predictive of differential treatment response.


We compared the efficacy of adalimumab, infliximab, ustekinumab, and vedolizumab for achieving endoscopic healing (EH) in the ileum and colon after one-year of therapy in Crohn’s disease (CD).
MethodsA pooled analysis of patient-level data from 344 patients with CD from four clinical trial programs was performed. Patients who received continuous adalimumab, infliximab, ustekinumab, or vedolizumab throughout the trial and had at least one ileocolonic segment with a Simple Endoscopic Score for CD (SES-CD) ≥ 3 at enrolment were included. Proportions of patients achieving one-year endoscopic healing (EH), defined as SES-CD of 0, using each of four biologics were compared. Multivariate logistic regression was used to model the relationship between individual biologics and one-year outcomes, adjusted for potential confounders of EH, including disease duration, concomitant corticosteroid use, and prior anti-TNF failure.
ResultsCompared to vedolizumab [10/77 (13%)], both infliximab [29/79 (36.7%), aOR: 3.27 (95% CI: 1.34-8.01), p<0.001] and adalimumab [12/40 (30%), aOR: 3.01 (95% CI: 1.10-8.21), p=0.032] were superior for achieving one-year EH of the ileum among patients with ileal involvement at baseline. No difference was observed between ustekinumab [5/22 (22.7%)] and vedolizumab [aOR: 2.75 (95% CI: 0.76-9.91), p=0.123]. In biologic-naïve patients, ustekinumab, adalimumab, and infliximab were superior to vedolizumab for achieving one-year EH of the ileum. For colonic disease, in comparison to ustekinumab [9/31 (29.0%), adalimumab [30/48 (62.5%), aOR: 4.04 (95% CI: 1.88-8.71), p<0.001] and infliximab (55/105 (52.4%), aOR: 2.02 (95% CI: 1.03-3.99), p=0.041] were superior for one-year EH in the colon among patients with colonic involvements at baseline. No difference was seen between vedolizumab [26/87 (29.9%)] and ustekinumab [aOR: 1.01 (95% CI: 0.39-2.59), p=0.987]. Similar differences were noted among biologic-naïve patients.


 Conclusion
ConclusionIn this post-hoc analysis of pivotal clinical trials, TNFα antagonists were generally superior to vedolizumab and ustekinumab for achieving EH of the ileum and colon in patients with CD. However, among biologic-naïve patients, ustekinumab, adalimumab, and infliximab were superior to vedolizumab for attaining one-year EH of the ileum.
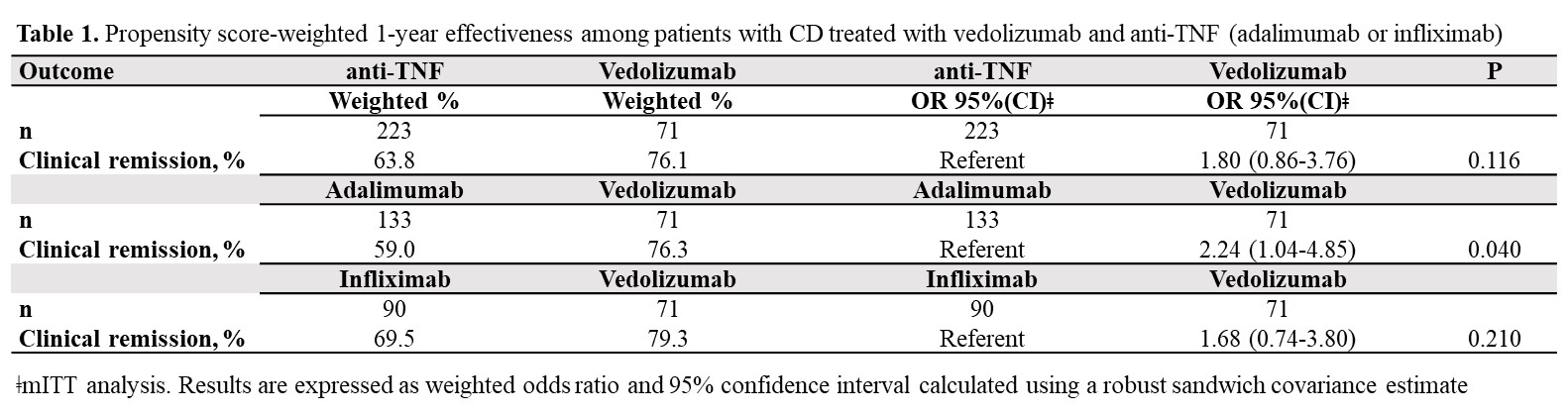
To gain insight into vedolizumab (VDZ) use as a first-line biologic in Crohn´s Disease (CD), this real-world study aimed to assess, within the maintenance phase, the 1-year comparative effectiveness and persistence of VDZ vs anti-TNF therapy in biologic-naïve CD-patients.
Between 2017-2020, 1200 consecutively enrolled biologic-naïve and biologic-experienced patients with ulcerative colitis (UC) and CD were prospectively included in the VEDOIBD-Registry from 45 IBD-experienced centres across Germany. 294 biologic-naïve CD-patients starting a new therapy with VDZ or anti-TNF (adalimumab: ADA or infliximab: IFX) were included in this real-world evidence (RWE) study. The Kaplan-Meier was used to summarize the treatment persistence from the start of therapy through week-52. The primary outcome was week-52 clinical remission (HBI ≤ 4). Patients were analyzed on a modified intent-to-treat basis (mITT; switchers considered as outcome failure) and on a per-protocol (PP) basis (excluding switchers). To reduce selection bias in the estimation of treatment effects, the inverse probability of treatment weighting propensity score (PS) was implemented. A weighted logistic regression was used to evaluate the effectiveness. The results were reported as odds ratio (OR) and 95% confidence interval (CI).
Results71 VDZ and 223 anti-TNF (ADA: 59.6%, IFX: 40.4%) biologic-naïve CD-patients were evaluated. 52-weeks after treatment initiation approximately 94% of VDZ patients were still in continuous treatment vs 75% of ADA and 78% of IFX (Figure 1). The mITT 1-year clinical remission rate was 76.1% for VDZ vs 63.8% for anti-TNF (OR: 1.80, 95% CI: 0.86-3.76). Similar results were observed for VDZ vs IFX (Table 1). In contrast, the clinical remission was significantly higher in the VDZ group than in the ADA group (OR: 2.24, 95% CI: 1.04-4.85). The PP analysis suggested comparative effectiveness, having excluded more anti-TNF switchers. 91.7% of week-14 responders VDZ patients were in clinical remission from week 14 through 52 vs 66.1% of anti-TNF patients (OR: 5.69, 95% CI: 1.66-19.5). Similar, significant, results were observed for VDZ vs ADA and for VDZ vs IFX (Table 2).
ConclusionIn this real-world setting comparing VDZ and anti-TNF in biologic-naïve patients via PS weighted analysis, VDZ showed especially in week-14 responders higher clinical remission rates in comparison to anti-TNF. The higher treatment persistence observed for VDZ, perhaps due to a more favourable safety profile vs anti-TNF, may be considered the main driver for the better effectiveness of VDZ at one year. These findings may aid physicians’ decision-making on the choice of VDZ as the first-line biologic for CD.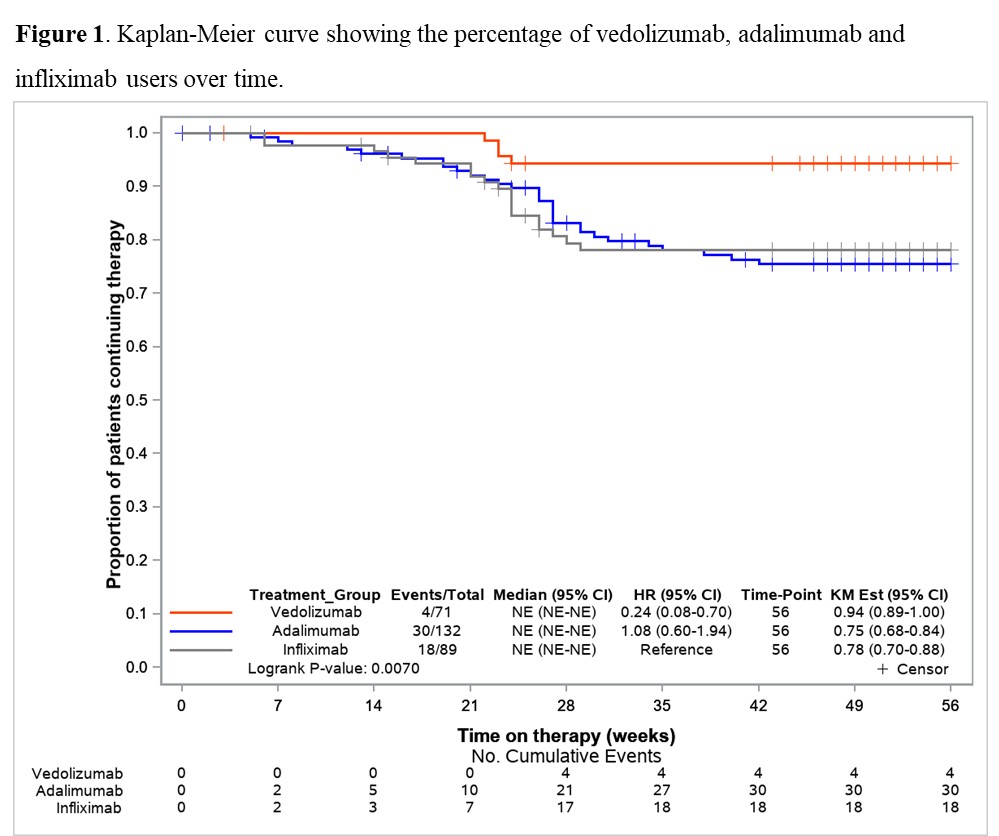

Main aim: To evaluate the retention rate of ustekinumab compared to vedolizumab in Crohn’s disease patients who failed anti-TNF therapy in clinical practice. Secondary aims: To compare the short-term and long-term effectiveness, and the safety of both treatments.
Methods755 patients were included (195 in the vedolizumab cohort and 560 in the ustekinumab cohort). After a median of 20 months (IQR 7.4-30) of follow-up, the survival rate for ustekinumab therapy was higher than vedolizumab (Figure 1). The propensity matching score verified the differences between both therapies. The short-term proportion of patients on clinical remission, steroid-free remission and clinical response was also superior in the ustekinumab cohort (Figure 2). In the long-term, significant differences were observed 2 years after the beginning of the treatments, although no differences in clinical response and remission rates were detected in patients who achieved clinical response at week 16 between both cohorts. Vedolizumab was discontinued in 142 patients and ustekinumab in 185, mainly due to primary non-response (52% in the vedolizumab and 58% in the ustekinumab cohort) and loss of response (34% and 25%, respectively) despite the fact that 35% of the patients required intensification. The predictive factors associated to the discontinuation of the therapy are described in table 1. Adverse events were observed, overall, in 12% of the patients, without differences between both groups (Table 2). Following the discontinuation of the treatment with vedolizumab/ustekinumab, other biologic agents were prescribed in 56% of the patients, and 27% underwent surgery.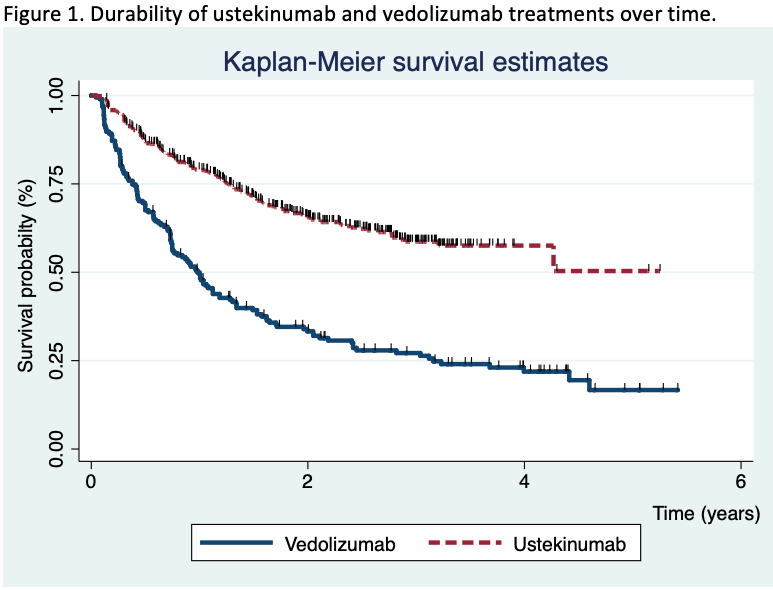



In clinical practice, a relatively high proportion of Crohn’s disease patients who received ustekinumab or vedolizumab for anti-TNF failure, maintained these drugs in the medium-long term, although ustekinumab retention rate was higher in comparison with vedolizumab.
The modified Rutgeerts' score (mRS) differentiates i2a – lesions confined to the anastomosis – and i2b – neoterminal ileum lesions – categories. Its relevance for therapeutic management of Crohn's disease (CD) patients after ileocolonic resection is still debated. Our objective was to compare the postoperative recurrence (POR) risk in patients with a mRS i2a or i2b score using an individual patient data meta-analysis.
MethodsWe conducted a systematic literature search of Medline, Embase and abstracts from international conferences (until July 2020) to identify all relevant studies reporting the risk of clinical and/or surgical POR and the i2a/i2b status in the year following ileocolonic resection. Initial datasets were obtained from the corresponding authors. Time from endoscopy to clinical and surgical POR was estimated using Kaplan-Meier method. The association between time to event and mRS was evaluated using a mixed Cox with centre as the random effect.
ResultsFrom the 17 studies identified, 7 published between 2008 and 2019 (cohort studies, n=4; clinical trials, n=2) corresponding to a total of 400 patients (median (InterQuartileRange) age at surgery 34 (26,47) years; 52% female) were included. In the year following ileocolonic resection, 189 (47%) patients displayed an i2a mRS and 211 (53%) an i2b. In the i2b group, we observed more male patients (56% versus 41%, p=0.01), more patients with previous ileocolonic resection (31% versus 21%, p=0.03) and temporary ileostomy (14% versus 6%, p=0.03) and an immunosuppressant or antiTNF therapy was more frequently initiated after endoscopy (42% versus 26%, p<0.01 and 36% versus 54%, p<0.01, respectively). The risk of clinical POR at 1, 3 and 5 years was 11% [6%-15%], 25% [18%-32%] and 36% [27%-43%] in the i2a group and 9% [5%-13%], 33% [26%-41%] and 47% [39%-56%] in the i2b group (p=0.63, p=0.12, et p=0.05 respectively). No significant difference was observed in terms of time to clinical POR (Hazard Ratio (HR)=1.27; Confidence Interval 95% [0.91,1.76]; p=0.16) (Figure 1) or surgical POR (HR=0.94; CI95% [0.44,2.00]; p=0.87). After exclusion of patients having initiated an immunosuppressant or a biologic in the 3 months after endoscopy (remaining cohort, n=361), no difference was observed in terms of clinical POR (HR=1.29 [0.92,1.80]; p=0.13) or surgical POR (HR=0.85 [0.39,1.84]; p=0.68).
In this individual patient data meta-analysis, no difference is observed between i2a and i2b mRS subcategories in terms of clinical, surgical or endoscopic POR. Limits of the mRS may explain this lack of predictive value.
Robust COVID-19 vaccine-induced antibody (Ab) responses are important for protective anti-viral immunity. Data are urgently needed to determine whether vaccine-induced immunity is impacted by commonly used immunosuppressive drug regimens in IBD.
MethodsWe prospectively recruited 447 adults (90 healthy controls and 357 IBD) at nine UK centres. The IBD study population was established (>12 weeks therapy) on either thiopurine monotherapy (n=78), infliximab (IFX) monotherapy (n=61), thiopurine & IFX combination therapy (n=70), ustekinumab (uste) monotherapy (n=56), vedolizumab (vedo) monotherapy (n=62) or tofacitinib (tofa) monotherapy (n=30). Participants had two doses of either ChAdOx1 nCoV-19, BNT162b2 or mRNA1273 vaccines. The primary outcome was anti-SARS-CoV-2 spike (S1 RBD) Ab concentrations, measured using the Elecsys anti-SARS-CoV-2 spike (S) Ab assay, 53-92 days after second vaccine dose, in participants without prior infection, adjusted by age & vaccine type. Secondary outcomes included proportions failing to generate protective Ab responses (defined cut-off anti-S concentration 15 U/mL, which correlated with 20% viral neutralization).
ResultsGeometric mean S Ab concentrations (figure 1) were lower in patients treated with IFX (153U/mL;p<0.0001), IFX and thiopurine combination (109U/mL;p<0.0001), tofa (430U/mL;p<0.0001) and uste (561U/mL;p=0.013) compared to controls (1596U/ml). No differences in S Ab concentrations were found between controls and thiopurine monotherapy-treated patients (1020U/mL;p=0.62), nor between controls and vedo-treated patients (944 U/mL;p=0.69). In multivariable modelling (figure 2), lower S Ab concentrations were independently associated with IFX (FC 0.10 [95% CI 0.07-0.14], p<0.0001), tofa (0.36 [95% CI 0.19-0.69],p=0.002) and uste (0.56 [95% CI 0.31-1.00],p=0.049), but not with thiopurine (0.77 [95% CI 0.54-1.11],p=0.17) or vedo (1.01 [95% CI 0.61-1.68],p=0.96). mRNA vaccines (3.67 [95% CI 2.72-4.96],p<0.0001) and older age (0.82 [95% CI 0.73-0.91],p=0.0003) were independently associated with higher & lower S Ab concentrations respectively. Protective Ab responses were generated by all thiopurine monotherapy, vedo, tofa and healthy control participants, but not by 11% of patients on IFX monotherapy, 13% on thiopurine & IFX combination therapy and 4% on uste.

COVID-19 vaccine-induced Ab responses are significantly reduced in patients treated with IFX, or tofa, and to a lesser extent with uste. No significant reduction was seen in vedo or thiopurine monotherapy-treated patients. Our data suggest that 3rd primary or booster vaccine doses for IBD patients might be tailored to an individual’s immunosuppressive treatment.
Financial support was provided as a Research Grant by Pfizer Ltd.